Never in its history has the nation’s family planning safety net faced as significant a threat as it does today. The policy agendas of the incoming presidential administration and the next Congress are being shaped by leaders adamant in their ideological opposition to—and intent to dismantle—the network of providers and the funding streams on which they rely that have comprised this country’s publicly funded family planning effort for decades. And foes of reproductive rights continue to dominate state legislatures and gubernatorial administrations.
Although the U.S. publicly funded family planning effort now hangs precariously in the balance, in many respects, this current threat started in the summer of 2015 with the public release of a series of deceptively edited videos seeking to discredit Planned Parenthood. The videos set off a renewed wave of federal and state-level attacks on all kinds of safety-net family planning funds and providers. Up until now, President Obama, his administration and the federal court system have served as a firewall, stopping a multitude of these harmful policies from taking effect.
Going into 2017, that firewall will likely fall, and it remains to be seen how the courts will respond to states’ ongoing attempts to undermine publicly funded family planning. At stake is the health of millions of low-income, young, immigrant and other underserved individuals who rely on the safety-net programs and providers for affordable contraceptive and related care. The potential harm to these individuals and families—and to society as a whole—is considerable.
Congressional Assaults
Threats to the family planning safety net are nothing new. For decades, foes of abortion rights—many of whom also oppose some or all forms of contraception—have claimed that any provider affiliated in any way with abortion should not receive public dollars, because those funds might somehow help women obtain abortions (see "‘Fungibility’: The Argument at the Center of a 40-Year Campaign to Undermine Reproductive Health and Rights," 2016). Moreover, antiabortion policymakers have often used this argument as cover to attack publicly funded family planning programs, a campaign that has made a high-profile return in the last two years.
In July 2015, antiabortion advocates released the first in a series of heavily edited videos orchestrated to publicly smear Planned Parenthood and to provide fodder for antiabortion lawmakers’ ensuing attempts to vilify and defund the organization. The fallout from the doctored videos was swift and severe. Only two weeks after the first video’s release, the U.S. Senate took the first of many congressional votes to disqualify Planned Parenthood health centers from eligibility for federal funds; some congressional efforts would have empowered states to take similar action. Since the summer of 2015, Congress has voted on the issue seven different times.
Notably, the vitriol against Planned Parenthood and abortion was not contained to defunding bills and votes. In October 2015, congressional leaders in the House formed a special panel charged with investigating Planned Parenthood’s clinical activities and funding sources—this, in addition to the four standing committees that have held hearings on Planned Parenthood’s business and clinical practices. Simultaneously, antiabortion lawmakers engaged in a separate but related legislative campaign to restrict the provision of abortion services.
In January 2016, after antiabortion lawmakers nearly forced a government shutdown over funding for Planned Parenthood, Congress sent a bill to the President’s desk in yet another attempt to defund the organization. In addition to repealing wide swaths of the Affordable Care Act, the bill would have excluded Planned Parenthood from federal funding sources, including Medicaid, for one year. That attempt, however, failed when President Obama stood firm and vetoed the bill. Still, the House would not give up and tried to override President Obama’s veto, but that vote fell short. Going into 2017, there remain no federal policies restricting public funding to Planned Parenthood as an organization.
Importantly, although not the main target of these recent congressional attacks, the Title X national family planning program has been negatively affected. Title X was originally passed in 1970 with strong bipartisan support, and Title X funds have been prohibited from going toward abortions since the program’s inception. Yet, since 2011, it has been perennially pegged for elimination by conservatives in the House, and Congress has cut funding to Title X by 10% since 2010, even as need for the family planning services Title X supports has increased by 5% over the same period.1
States Join the Fray
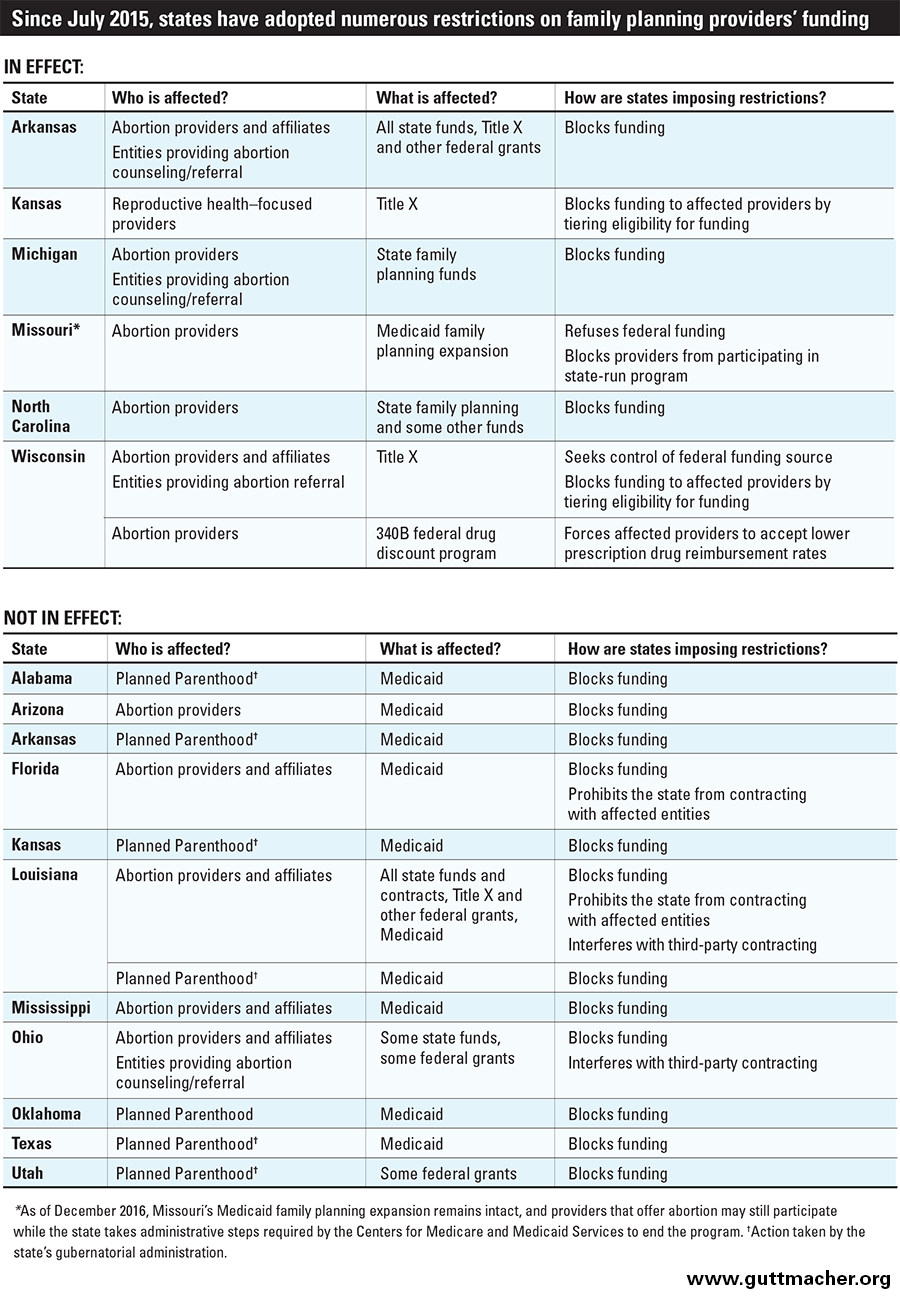
Policymakers’ attempts to restrict family planning funds and providers have been reinvigorated not just in Congress, but across many states. Of course, this most recent wave of state funding restrictions is not new either. Many state policymakers have been looking to defund publicly supported family planning for decades (see "Efforts Renew to Deny Family Planning Funds to Agencies That Offer Abortions," February 2002). As with other campaigns to limit access to reproductive health care, states have had more success than Congress in actually passing and implementing policies restricting family planning funding. Before 2015, 11 states had such restrictions in place; since July 2015, 24 states have tried and 15 have succeeded in adopting some kind of funding restriction, although many have been tied up or struck down in court and are, therefore, not in effect (see table). The entities being targeted, the funding streams that could be affected and the policy tactics lawmakers are employing all vary from state to state and are ever-evolving.
Who Is Affected?
In the wake of last summer’s smear videos, many antiabortion state policymakers have sought to specifically exclude otherwise-qualified Planned Parenthood health centers from publicly funded programs, including those Planned Parenthood sites that do not offer abortion. Other policies look to exclude any entity that provides abortions, or any family planning provider that is formally affiliated with such an entity; this typically affects safety-net health centers that focus on reproductive health care, rather than primary care, including—but not limited to—Planned Parenthood.
In some cases, states are now looking to go so far as to exclude from state-administered funding all entities that simply offer abortion counseling or referrals at a client’s request. Importantly, these restrictions clash with medical standards, as well as the federal regulations governing the Title X program that explicitly require participating sites to offer nondirective pregnancy-options counseling and referral for all options, including abortion.
What Funds Are Affected?
The most common and long-standing target for these attacks at the state level are family planning funds. These funds come in multiple varieties: state-only funding directed toward family planning services for underserved communities, federal funding controlled by the state (e.g., Title X grants awarded to a state agency), and mixtures of state and federal funding (e.g., coverage of family planning services provided through Medicaid). Medicaid is by far the largest source of the public investment in family planning services, accounting for 75% of these funds.2 And a few states have targeted Medicaid programs specific to family planning services; these so-called Medicaid family planning expansions have been implemented by about half the states to expand eligibility for contraceptive and related care for low-income individuals not otherwise eligible for full-benefit Medicaid.3
Especially in this most recent wave of restrictions, some state policymakers are so motivated to shut down certain providers that they are looking not only to exclude them from family planning–specific funds, but also from other public programs that might support providers’ work in their communities. Such targeted funds are intended to address a wide range of public health concerns, including infant mortality, STIs, breast and cervical cancer, and violence against women. Even programs that connect low-income families with cash and nutritional assistance have been a target of these restrictions.
How Are States Imposing Restrictions?
States have attempted to pull these various forms of funding out from under the family planning safety net using many different policy tactics. Most directly and commonly, states have sought to exclude specific types of providers from receiving certain types of public funds.
In other cases, states have implemented policies that disadvantage certain providers in the state’s allocation of public funds through a process often referred to as "tiering." Ultimately, tiering has the same effect of denying public support to disfavored organizations, while enabling policymakers to argue that the policy merely rewards "worthy" organizations—most often, public health departments or safety-net providers that offer family planning services in the broader context of primary care.
State policymakers have also tried to take full control of a given program, giving the state authority to either ban certain providers outright from those funds or to impose a tiering system. Some states have used this approach with federal Title X grants that might otherwise go to a nonprofit organization unaffiliated with the state government. Others have sought full control of a Medicaid family planning expansion program, forgoing federal funding in favor of gaining the autonomy to exclude certain providers on ideological grounds.
Finally, several states have resorted to the most extreme but straightforward tactic: getting rid of a funding source entirely, such as by cutting a state’s allocation for family planning from its annual budget. Policymakers might take this approach after others have been barred by the federal government or by the courts. For example, the Missouri legislature eliminated the state’s entire family planning program in 2003 after earlier attempts to prevent organizations that provide or refer for abortion services from receiving state family planning funds were repeatedly struck down by the courts.
State Examples
Over the past several years, states have pieced together these tactics in numerous ways as a means of dismantling the family planning safety net. For instance, Michigan’s 2016 budget bill reenacted a ban on state family planning funds from going to organizations that provide abortions, or offer abortion referrals or counseling. And a 2016 law enacted in Louisiana that is currently blocked by the courts prohibits all federal, state or local funds—including Title X grants, Medicaid and state contracts—from going to abortion providers. The law also seems to prohibit any type of third-party entity under contract with the state from entering into its own, separate contract with an abortion provider.
A new law enacted in Wisconsin directs the state’s health department to compete for Title X grant funding; for years, the state’s Title X grant has been awarded to the state’s Planned Parenthood affiliate. If the state’s bid is ever successful, Title X dollars are to be distributed among safety-net providers in the state according to a tiered system: Health centers operated by the state or localities would be given priority, followed by community health centers. Providers that offer abortion services or are affiliated with a provider that does so would be ineligible, as would any entity that makes abortion referrals—a direct violation of the federal regulations governing the Title X program, which require Title X–funded sites to offer nondirective pregnancy-options counseling and referral.
Another recent example can be found in Ohio, where the legislature passed a sweeping new law—subsequently struck down in court—that would have ensnared any entity that offers, counsels on or refers for abortion, as well as organizations affiliated with such entities. It would have explicitly excluded affected entities from participating in a number of specific federal programs, including grants to prevent violence against women and connect those experiencing violence to much-needed services; expand screenings for breast and cervical cancer, and HIV; prevent infertility; and offer comprehensive sex education to public school students. (Title X funds would not have been affected.) The law also would have prohibited third-party entities that receive affected funds from separately contracting with any entity offering or affiliated with abortion services, counseling or referral.
In yet another vein of defunding attempts, 15 states in the last two years have moved to limit safety-net family planning providers’ eligibility for reimbursement under Medicaid. These attacks have come via both gubernatorial administrations and legislatures, and typically target Planned Parenthood. Arizona, for example, passed a law in 2016 that allows the state’s Medicaid program to exclude any provider that receives any type of public funding and also provides abortion, or is affiliated with a provider that does so. The law is not currently in effect; the state and Planned Parenthood reached an agreement that Arizona will not enforce the law until accompanying regulations are developed, at which time Planned Parenthood has reserved the right to file a new legal challenge. In fact, to date, none of these efforts to exclude providers from Medicaid have gone into effect because of successful legal challenges and emphatic push-back from the Obama administration.
Policymakers’ attempts to restrict family planning funds and providers have
been reinvigorated not just in Congress, but across many states.
Also on the Medicaid front, Missouri’s 2017 budget bill moves to end the state’s Medicaid family planning expansion program, forgoing the federal support it provides—$9 for every state dollar spent, approximately $8.3 million in Missouri—and instead funding its family planning initiative entirely with state dollars.4 State legislators assert that forgoing federal dollars would give them the latitude to ban Planned Parenthood from participating. Currently, the joint federal-state program and reimbursements to Planned Parenthood under that program remain intact; the federally mandated process for a state to withdraw takes months, including a public comment period and a requirement that the state offer a plan as to how it will ensure continued accessibility of family planning services. Missouri is following a path first set out by Texas in 2011 (see "The State of Sexual and Reproductive Health and Rights in the State of Texas: A Cautionary Tale," Spring 2014).
As a final example, in 2016, the Wisconsin legislature implemented yet another, relatively new type of restriction on safety-net family planning providers that also offer abortion: limiting these providers’ drug reimbursement rates under Medicaid. The federal 340B Drug Pricing Program helps participating safety-net centers to obtain prescription drugs at reduced rates from pharmaceutical manufacturers, in turn enabling these sites to more readily absorb the cost of providing contraceptives at little or no cost to their clients. Wisconsin’s new law moves much of the 340B savings for which affected safety-net family planning sites are eligible over to the state Medicaid program itself, with the intent to curb these providers’ ability to stock and dispense affordable contraceptive methods.
The Threats Ahead
Under President Obama, the federal government has strongly and consistently pushed back against attempts to undermine family planning funds and providers. For example, in December 2016, the administration finalized new regulations to stop states from directing Title X funds away from reproductive health–focused providers. Furthermore, the Obama administration has vehemently rejected states’ attempts to deny Medicaid reimbursements to Planned Parenthood and other providers associated with abortion, most prominently in an April 2016 letter to state officials.5,6 The letter made clear that such efforts are in violation of federal law, which guarantees enrollees a free choice of qualified providers for family planning care. Federal courts have thus far agreed with this interpretation of the law, consistently striking down states’ attempts to disqualify Planned Parenthood and similar providers from their Medicaid programs.
Following the results of the 2016 elections, however, this federal firewall is at risk of failing, putting the nation’s family planning safety net very much in danger. In November, President-elect Trump named Rep. Tom Price (R-GA) to lead the Department of Health and Human Services, a choice sharply criticized by reproductive rights and public health groups. Price, an outspoken opponent of abortion rights, was the lead sponsor of legislation that would have barred federal funds from Planned Parenthood were it not vetoed by President Obama. Price also recently signed onto a congressional letter opposing the Obama administration’s new protections for the Title X program. Trump’s choice appears to send a signal that his administration will not stand in the way of state funding restrictions that fly in the face of federal law and will likely support congressional attacks on Title X, Medicaid and safety-net family planning providers, particularly Planned Parenthood.
The potential impact to the millions of individuals who rely on these programs and providers is especially troubling given the increasing need for publicly funded family planning services: Nearly one million more women were in need of such care in 2014 compared with 2010, with particularly large increases among poor and Hispanic women.1 All told, more than 20 million U.S. women are now in need of publicly funded family planning care. Antiabortion state policymakers and members of Congress alike should heed this reality and, instead of trying to tear down the safety net, turn to bolstering publicly funded family planning programs and providers nationwide.