Over the past two years, antiabortion members of Congress and state policymakers have fervently pursued a political and policy agenda to deny public funding to Planned Parenthood. This concerted effort seeks to exclude Planned Parenthood health centers from state and federal funding streams, including the Title X national family planning program and Medicaid, and carries the potential to deprive women of the contraceptive services and counseling, STI testing and treatment, and breast and cervical cancer screenings that Planned Parenthood provides.
Although the Obama administration and federal courts have largely stopped these defunding attempts, the Trump administration and the 115th Congress are expected to give defunding attempts new traction. Notably, President-elect Trump’s nominee for Secretary of the Department of Health and Human Services, Rep. Tom Price (R-GA), is a vocal opponent of abortion and Planned Parenthood (see "Recent Funding Restrictions on the U.S. Family Planning Safety Net May Foreshadow What Is to Come," 2016).
Attacks on Planned Parenthood seek to undermine a network that has capably served millions of women for decades. Although proponents of defunding Planned Parenthood argue that other providers—namely health departments and federally qualified health centers (FQHCs)—would easily be able to fill the overwhelming hole torn in the safety net, evidence suggests otherwise.1 Planned Parenthood health centers consistently perform better than other types of publicly funded family planning providers on key indicators of accessibility and quality of contraceptive care.2 Plus, Planned Parenthood serves a greater share of women who obtain contraceptive care from safety-net health centers.3 And in some communities and for many women, Planned Parenthood is the sole source of publicly funded contraceptive care.3,4 It is simply unrealistic to expect other providers to readily step up and restore the gravely diminished capacity of the family planning safety net were Planned Parenthood defunded.
Women can often obtain care more quickly from Planned Parenthood. Sixty-two percent of Planned Parenthood health centers offer same-day appointments, a proportion similar to FQHCs (58%), but higher than health departments (42%).2 Moreover, the average wait for an initial contraceptive appointment at a Planned Parenthood health center is 1.2 days, while the average wait time for such a visit is 2.5 days at sites operated by FQHCs and 4.1 days for health department sites.
Planned Parenthood health centers are also by far the most likely to accommodate clients who have difficulty taking time off from work or family responsibilities to obtain care: Seventy-eight percent of Planned Parenthood health centers offer extended evening or weekend hours versus 57% of FQHCs and just 18% of health departments.2
Planned Parenthood health centers facilitate women’s timely access to a wide range of methods. Planned Parenthood is particularly good at ensuring a woman can choose the contraceptive method that will work best for her, and helping clients to start and effectively use their chosen method (see chart 1).2
First, Planned Parenthood centers are considerably more likely to offer a broad range of contraceptive methods than sites operated by other types of agencies. Nearly all Planned Parenthood health centers offer the full range of Food and Drug Administration (FDA)–approved reversible contraceptive methods, compared with about two-thirds of health departments and half of FQHCs.2
Second, Planned Parenthood makes it easier for women to obtain highly effective long-acting reversible contraceptive (LARC) methods. Nearly all Planned Parenthood centers offer insertion of IUDs and implants on the same day as a client’s initial appointment, a drastic difference from both health departments and FQHCs.2
Third, Planned Parenthood sites are particularly likely to help women who choose oral contraceptives to get their pill supply without having to make an additional trip to a pharmacy. The vast majority of Planned Parenthood health centers offer initial oral contraceptives and refills on-site, as do three-quarters of health department sites; only one-third of sites operated by FQHCs do so.2 In addition, 99% of Planned Parenthood health centers allow women to delay a pelvic exam when initiating hormonal contraceptives and use the "quick-start" protocol to enable a client to start the pill on the day of her visit, regardless of where she is in her menstrual cycle.
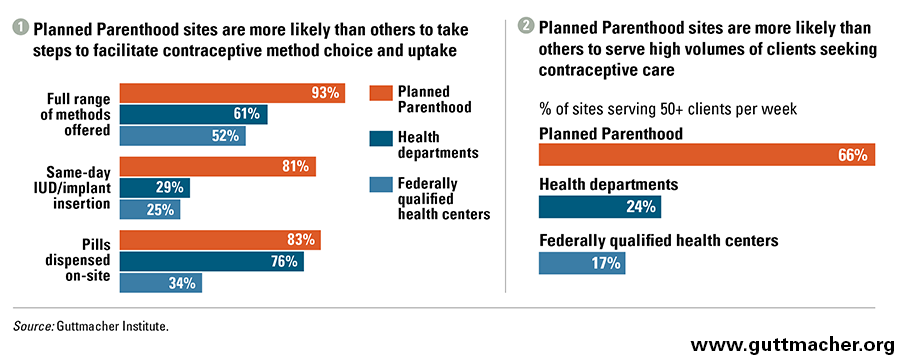
Moreover, because of their comparatively large client load, Planned Parenthood sites serve a disproportionate share of clients. Despite the fact that Planned Parenthood sites accounted for only 10% of all publicly funded family planning clinics in 2010 (the last year for which data are available), they served 36% of publicly funded contraceptive clients that year.3
Planned Parenthood is an important source of care for many women. In 332 of the 491 counties that Planned Parenthood health centers served in 2010, Planned Parenthood served at least half of the women obtaining publicly supported contraceptive services from a safety-net health center.5,6 In 103 of these counties, Planned Parenthood sites served all of these clients. Nearly one-third of all women in need of publicly funded contraceptive services lived in the 332 counties where Planned Parenthood served all or most safety-net family planning clients.
A 2016 survey of clients at Title X–funded health centers reinforces the importance of Planned Parenthood to the women it serves. Twenty-six percent of clients at a Planned Parenthood site reported that it was the only place they could get the services they need.4
Planned Parenthood’s critical role in meeting the need for publicly funded contraceptive care cannot be overlooked. This is especially true given that the need for such care is on the rise: In 2014, 20.2 million U.S. women were in need of publicly funded family planning services—an increase of 5%, or one million women, since 2010.7
Unfortunately, it seems likely that antiabortion policymakers will disregard this very real need in their communities and continue their myopic campaign to defund Planned Parenthood in the coming year. Although it is difficult to predict exactly how potential restrictions on Planned Parenthood’s eligibility for various public programs might play out, it is highly doubtful that other providers could step up in a timely way to serve the millions of women suddenly left without their preferred, and sometimes only, source of care. It is also unclear whether other types of safety-net health centers would be able to consistently provide the same degree of accessible, high-quality contraceptive care offered by Planned Parenthood.
What we do know is that women nationwide rely on Planned Parenthood health centers for the contraceptive and related services they need. For many who are low-income or young, who are immigrants or who find themselves uninsured, losing Planned Parenthood means losing a trusted provider, and in some cases, the only source of care they have.