Medicaid has long been vital to family planning care in the United States. In 2015, the program covered 20% of women aged 15–44, including 48% of those living below the federal poverty line.1 Federal Medicaid requirements ensure that all enrollees have coverage for family planning services without any copayments, free from coercion and at the qualified provider of their choice.2 And because it provides millions of people with family planning coverage, Medicaid accounts for three out of every four public dollars spent on family planning nationwide.3
Conservatives in Congress and the Trump administration are working to fundamentally restructure Medicaid in ways that could undermine coverage overall and for family planning in particular (see "Why Protecting Medicaid Means Protecting Sexual and Reproductive Health," 2017). States can and should take steps to preserve Medicaid’s coverage and protections for family planning services, and even make this coverage better for the millions of low-income individuals who rely on it.
Choice of Services
Federal law, along with federal agency regulations and guidance, includes strong protections for Medicaid enrollees that are designed to ensure they can choose contraceptive methods and other family planning services that best fit their needs, without financial or administrative barriers. These protections are in danger at the federal level, such as through potential changes to regulations and guidance issued by the Centers for Medicare and Medicaid Services (CMS) or through legislation that could convert Medicaid into a block grant program, which would eliminate a vast array of protective federal Medicaid rules. States can and should work to counter this danger by codifying these protections into their own laws and regulations, and in the process, take the opportunity to make them even stronger.
Cover All Family Planning Care
Since 1972, federal law has required state Medicaid programs to cover family planning services and supplies for all reproductive-age enrollees. However, there is no clear federal definition of what constitutes family planning services and supplies. For enrollees eligible under the Affordable Care Act’s (ACA) Medicaid expansion for low-income adults, the program must, at the least, cover contraceptive counseling and services and all female contraceptive methods that have been recognized by the U.S. Food and Drug Administration (currently, 18 of them).4 For other Medicaid enrollees, CMS has not required a specific list of methods, but in a 2016 letter to state officials, the agency recommended that states cover all of them, asserting that "patient choice and efficacy should be the principal factors used in choosing one method of contraception over another."5
States should codify the requirement for Medicaid to cover family planning services and supplies. Moreover, they should go beyond that by requiring that all Medicaid enrollees receive coverage for all contraceptive methods. That should include the 18 methods currently used by women, as well as the two methods—vasectomy and male condoms—used by men, along with any future methods. States should also specifically include coverage of methods provided over the counter without a prescription, in addition to prescription and surgical methods, as well as counseling, follow-up care, and all needed services related to starting, ending or switching methods (such as removal of an IUD or implant). States should apply these and other protections to all Medicaid enrollees, whether covered directly by the state or through a Medicaid managed care plan run by a private-sector insurer.
States should also bolster Medicaid coverage of important family planning–related services by requiring coverage for the full range of preventive care detailed in federal guidelines for the provision of quality family planning services.6,7 That includes counseling, screening and other care related to HIV, other STIs, cervical cancer, intimate partner violence and more.
Prohibit Cost-Sharing and Other Restrictions
States should explicitly bar the application of utilization control techniques for family planning, including:
- copayments, deductibles and other patient out-of-pocket costs;
- prior authorization (requiring permission from the state or a plan before a clinician can provide a given method or service);
- step therapy (requiring that a patient try and fail with one method before trying the method of her choice);
- policies that restrict a change in method (such as refusing to reimburse for the removal of an IUD or contraceptive implant); and
- inappropriate quantity limits (such as covering only one IUD every five years, even if a previous device was expelled or removed for a planned pregnancy).
Again, this would codify and build on current federal policy. Federal law prohibits cost-sharing for family planning under Medicaid. CMS regulations require that Medicaid enrollees be "free from coercion or mental pressure and free to choose the method of family planning to be used."8 In regulations and guidance to states in 2016, CMS interpreted that requirement to prohibit step therapy for contraception, require coverage of contraceptive device removal and discourage inappropriate contraceptive quantity limits.2 CMS also severely limited the use of prior authorization for family planning by clarifying that patients must be free to choose a method based on criteria such as side effects, clinical effectiveness, whether the method is reversible, and ease of use.
Protect Patient Confidentiality
States should also take steps to promote confidentiality as another family planning–related protection for Medicaid enrollees. Many routine communications to enrollees in Medicaid—particularly those related to enrollment, renewal, billing and reimbursement—can inadvertently violate patient confidentiality, which may be particularly problematic for sensitive care such as family planning.9
States, managed care plans and health care providers are required under current federal regulations to accommodate a Medicaid enrollee’s request to communicate via alternative means or at an alternative location (such as via e-mail rather than by paper mail delivered to her home address). States should codify this protection and strengthen it by proactively asking patients about their communication preferences. They should also review the standards and systems in place at state agencies and at managed care plans to identify and address potential violations of confidentiality. For example, they could require plans to suppress automatic notices that might accidentally reveal that a Medicaid enrollee received sensitive services.
Choice of Providers
Federal Medicaid policy has paired strong protections for family planning coverage with strong protections for enrollees’ ability to access that care. Conservative policymakers have sought to undermine these protections, most notably by trying to deny Medicaid reimbursement for family planning and related services to Planned Parenthood health centers and other providers that either offer abortion-related services or are affiliated with a provider that does so.10
Ensure In-Network Access
States should help protect access to providers by establishing strong "network adequacy" standards for Medicaid managed care plans. For family planning, this means requiring plans to contract with a wide network of safety-net health centers, as well as clinicians—both physicians and advanced practice clinicians—who specialize in obstetrics and gynecology.
Doing so would implement and build on 2016 federal regulations that require provider networks that are extensive enough to meet enrollees’ needs for obstetrician-gynecologists and family planning providers. As CMS noted, in-network access is important because "use of network providers facilitates claims payment, helps enrollees locate providers more easily, and improves care coordination."11
Ensure Out-of-Network Access
As a parallel measure, states should act to protect access to care outside of managed care provider networks, and for enrollees who are not in a managed care plan at all. Specifically, they should codify enrollees’ right to a free choice of any qualified provider for family planning services—even for enrollees in a managed care plan that otherwise restricts their insurance coverage to a limited network.
Further, states should make it clear that because of this protection, enrollees cannot be required to obtain a referral for family planning care, regardless of whether the provider is in network or out of network. They should provide Medicaid enrollees with clear and timely instructions for how to access this care, and require Medicaid managed care plans to do the same. All of these protections are currently required under federal law and regulations.
Protect Providers from Discrimination
In protecting Medicaid enrollees’ choice of providers, states should also make it clear that they are protecting those providers from discrimination in their ability to participate in Medicaid. States should reaffirm that—as stated in a 2016 CMS letter to state officials—enrollees cannot be denied access to a provider solely because they offer the "full range of legally permissible gynecological and obstetric care, including abortion services."12 States should also make it clear that plans cannot discriminate against safety-net family planning providers in other ways, such as by failing to provide timely or appropriate reimbursement for their services.
The 2016 CMS letter came in response to attempts by numerous governors and state legislatures to bar Medicaid reimbursement to Planned Parenthood affiliates and other safety-net providers. Federal courts have sided with CMS’s interpretation of Medicaid law in every case decided so far. Yet, conservatives at the federal and state levels have persisted in their efforts, and it seems unlikely that CMS will continue to stand by its current interpretation of the law under the Trump administration.
Ensure Adequate Reimbursement
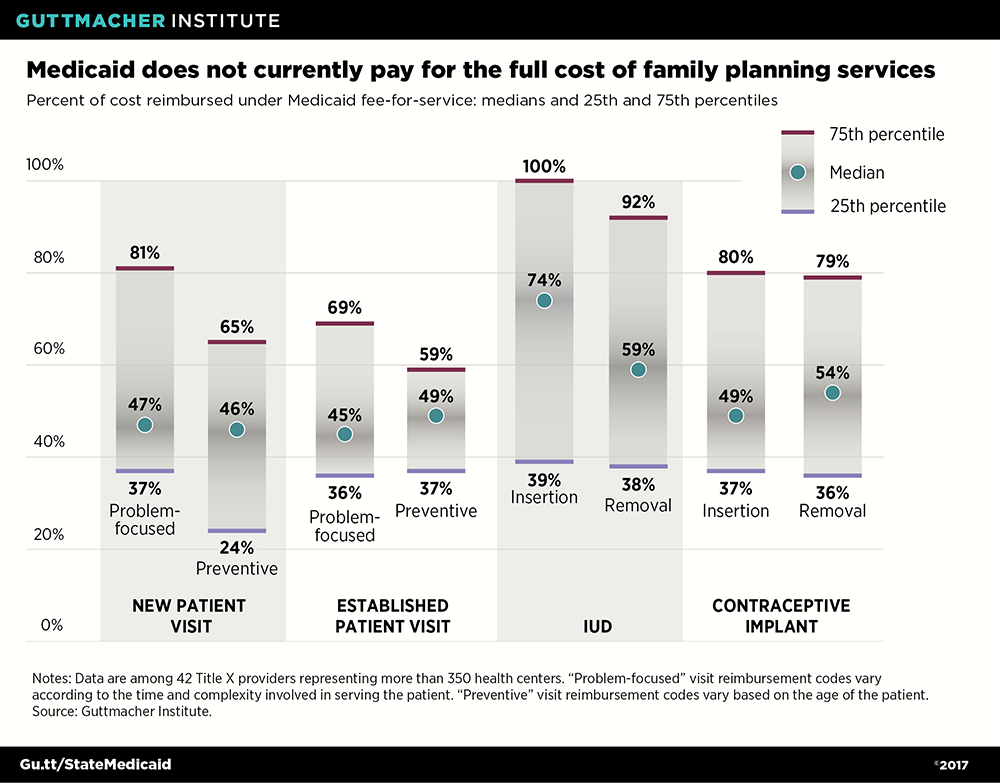
States should also set sufficient reimbursement rates, and require managed care plans to do the same, so that family planning providers can afford to provide quality care under Medicaid. This would be in line with current federal law, which requires reimbursement rates sufficient to ensure an adequate Medicaid provider network. In practice, low reimbursement rates have led many private providers to refuse to take on Medicaid patients at all.13 Title X providers and other safety-net family planning centers, by contrast, must accept all patients, regardless of their ability to pay, and they routinely struggle with inadequate reimbursement. A 2016 Guttmacher Institute analysis found that Medicaid reimbursement for family planning services provided by Title X clinics typically covers less than half the actual cost of these services (see chart).14
Protect Against Religious Refusals
As a final step to ensure access to providers, states should revisit their protections and procedures for responding to the religious and moral objections of providers and plans. The goal should be to ensure that—despite any objections on the part of providers or plans to certain services, referrals or information—enrollees are never denied or delayed in receiving family planning and other reproductive health care that Medicaid covers.
For example, states should codify and build on limited federal protections for Medicaid enrollees by:
- ensuring that plans clearly inform enrollees and potential enrollees about Medicaid-covered services that the plan itself does not cover;
- enforcing plans’ obligation to ensure enrollees’ access to all services under their contract, even when network providers have objections;
- ensuring that enrollees may switch managed care plans at any time in response to plans’ or providers’ religious or moral objections;
- establishing a toll-free hotline and an online portal through which enrollees could learn how and where to obtain needed care not covered by plans;
- requiring plans and providers to direct patients to state-run information resources when needed; and
- informing enrollees of their rights on a recurring basis.
Eligibility for Coverage
Protections for Medicaid enrollees’ choice of services and providers are only meaningful if people are eligible for coverage in the first place and can get and stay enrolled. Although conservatives in Congress and the Trump administration are looking to scale back eligibility and enrollment—by phasing out the ACA’s Medicaid expansion, instituting caps on federal Medicaid spending or setting up new eligibility restrictions—states can and should act as a countervailing force.
Expand Medicaid Eligibility Under the ACA
Currently, there are 19 states that have not yet expanded Medicaid to cover low-income adults under the ACA.15 The option to expand coverage remains on the table, and several states have started to consider it again seriously. For example, the Kansas legislature passed a Medicaid expansion bill in 2017, and only narrowly failed to override a veto by Gov. Sam Brownback (R).16 Policymakers in Georgia, Maine, North Carolina, Utah and Virginia are also reportedly looking to revive expansion efforts.17 If states succeed in expanding Medicaid, that would provide full-benefit health coverage—including family planning coverage—for potentially millions of currently uninsured people.
Expand Medicaid Eligibility for Family Planning
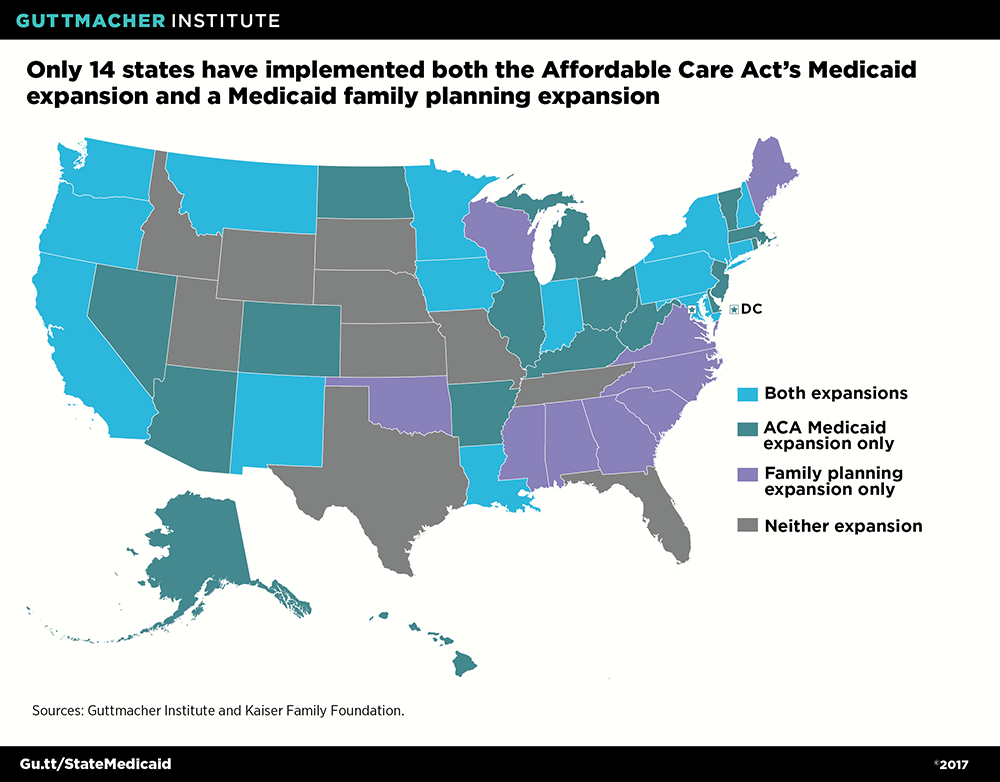
Another option for states is to expand Medicaid in a more targeted way: by extending eligibility specifically for family planning services to individuals otherwise ineligible for Medicaid. States can do so either under a provision of the ACA (via a "state plan amendment") or through a research and demonstration "waiver" of federal law. About half of states have expansions in place today (see map).18
Those states that do not have an expansion in place—including several states that have rolled back expansions in recent years—should reconsider. Numerous studies have documented that Medicaid family planning expansions improve access to care, help women avoid unintended pregnancies and save considerable amounts of public funds by helping states avoid costs for maternity and infant care related to unwanted pregnancies.19 Moreover, these expansions can provide a limited safety net for state residents—albeit for family planning and related services only—if full-benefit coverage via Medicaid or the private insurance marketplaces is inaccessible or unaffordable.
Resist Eligibility Restrictions
One final way that states should protect Medicaid eligibility is by declining what may appear at first to be tempting offers by Congress and the Trump administration. For example, if Congress offers states increased authority to shape their Medicaid programs in exchange for a cap on federal spending, state policymakers must consider the potential consequences for Medicaid enrollment and coverage. The impact of capping federal expenditures would escalate over time as spending failed to keep up with inflation. That would increase financial pressure on states to scale back eligibility, coverage and provider reimbursement, and leave Medicaid less responsive to economic crises, rising costs and changing health care needs.20
Similarly, states should resist federal offers to impose punitive restrictions on Medicaid eligibility, such as work requirements for many enrollees, lock-out periods for enrollees who miss their premium payments and lifetime limits on how long an individual can be covered under Medicaid. These types of restrictions—which the Trump administration has promoted as options via Medicaid waivers—are based on negative stereotypes about the people who rely on Medicaid, overestimate the availability and affordability of employer-sponsored coverage, and ignore the reality that Medicaid can help people get and stay healthy enough to work.21
Family Planning Matters to Medicaid
States should take all of these steps to protect and enhance Medicaid’s coverage of family planning care because family planning promotes the central goals of Medicaid. First, family planning services are effective preventive services that improve the health of women and their children—and improving health is Medicaid’s most basic goal. By helping women to avoid unintended pregnancies, contraceptive use decreases pregnancy-related illness, injury and death, especially for women who have medical conditions that may be exacerbated by pregnancy.22 And by helping women to plan and space wanted pregnancies, contraceptive use can help reduce the risk of having a premature or low-birth-weight delivery. In addition, pregnancy planning can help women address chronic conditions before they become pregnant and start prenatal care as early as possible in pregnancy. Moreover, the other preventive services offered as part of a family planning visit can help people avoid or address HIV and other STIs, infertility, cervical cancer, intimate partner violence and other negative health outcomes.
Second, family planning care contributes to Medicaid’s goal of helping individuals and families be independent and self-sufficient. There is considerable evidence to document that family planning care helps people complete their education, get and keep a job, earn a better wage, and support themselves and their families.22 In doing so, it has advanced women’s equality and social justice in the United States.
Finally, Medicaid coverage of family planning services helps to reduce unnecessary medical costs, thereby contributing to another key Medicaid goal—operating an efficient program. Contraception, screening for HIV and other STIs, screening and vaccination related to cervical cancer, and other family planning services help to prevent avoidable and potentially expensive health problems. All told, publicly funded family planning services, including those funded by Medicaid, save $7 for every public dollar spent.23
In sum, family planning care promotes the health and the social and economic well-being of women, families and society. States should take every step possible to protect and improve coverage of these services under Medicaid—regardless of what Congress and the Trump administration may do.