Key Points
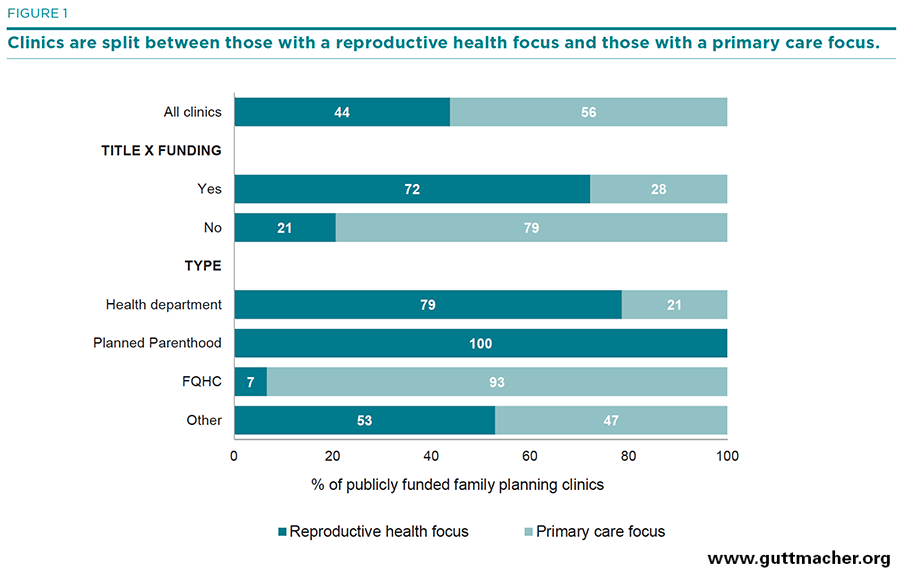
- Publicly funded family planning clinics provide critical contraceptive, sexual and reproductive health and other preventive health services to poor and low-income women.
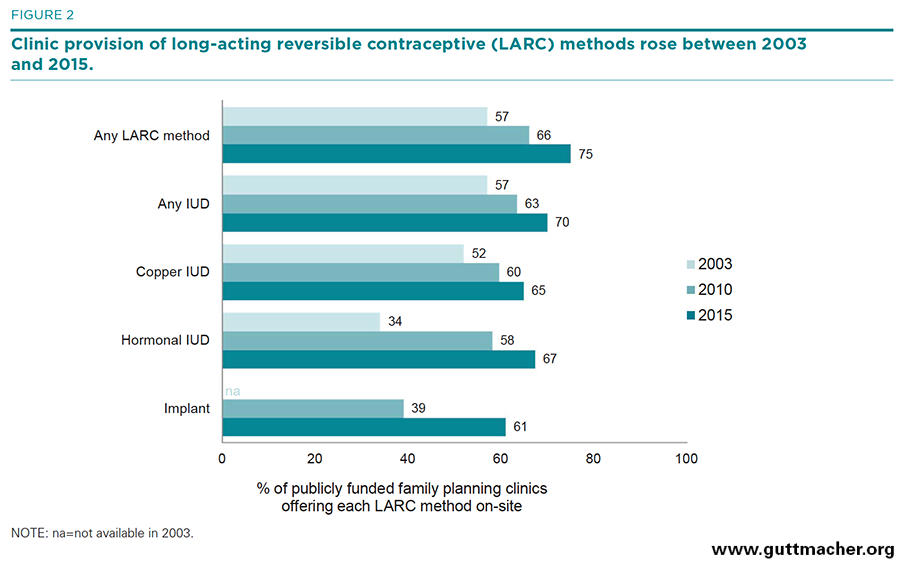
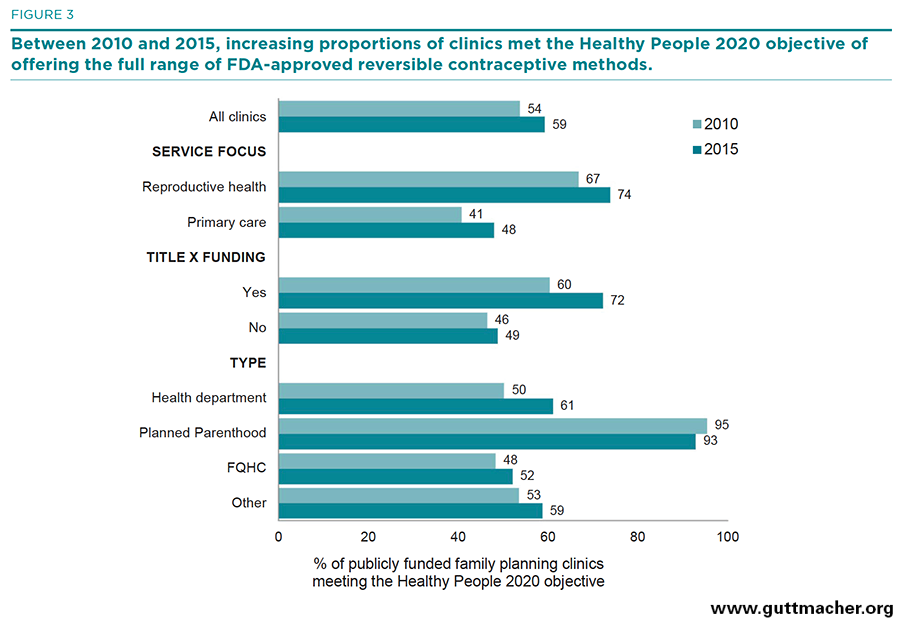
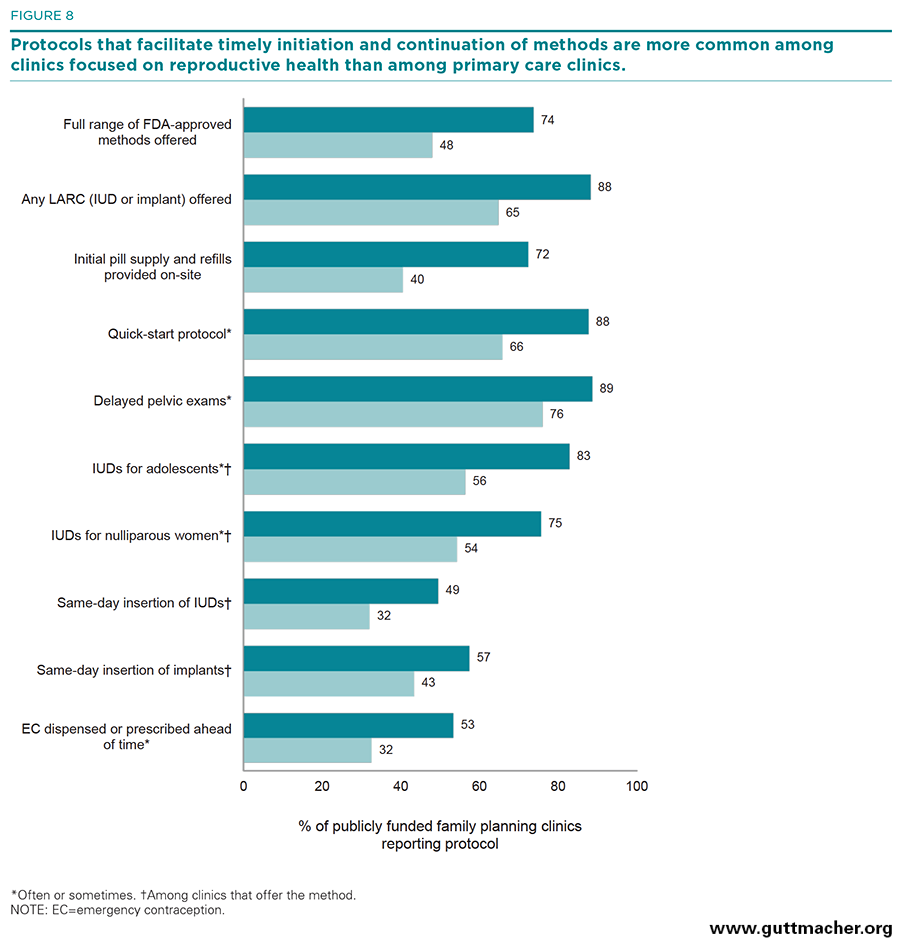
- Between 2010 and 2015, the proportion of these clinics offering a wide range of contraceptive methods on-site, especially long-acting reversible contraceptive (LARC) methods, increased significantly. More than half (59%) of clinics met the Healthy People 2020 objective of offering the full range of contraceptive methods.
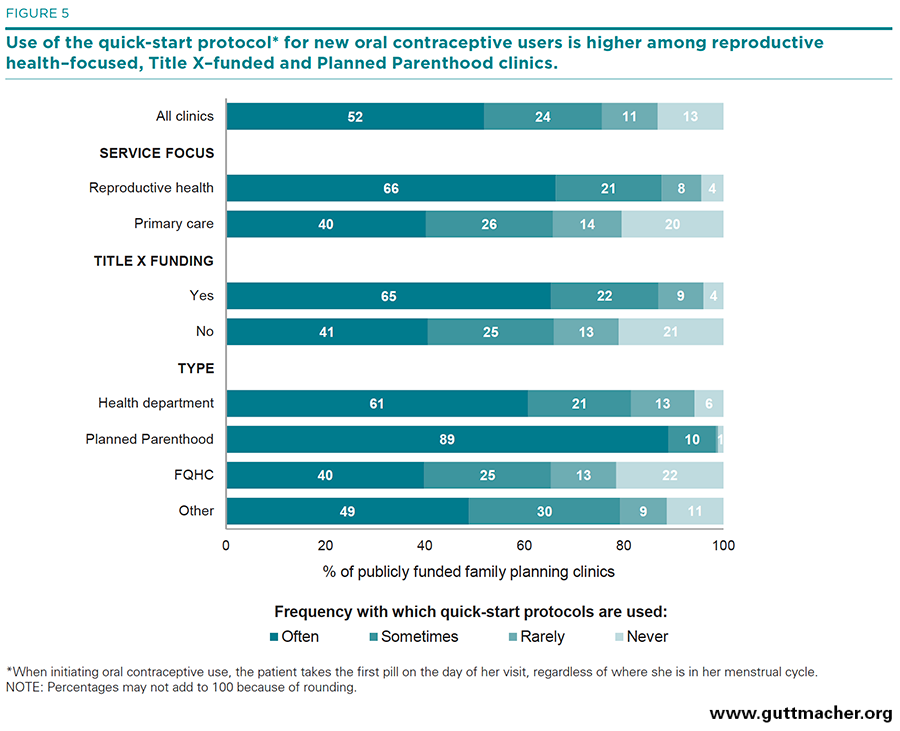
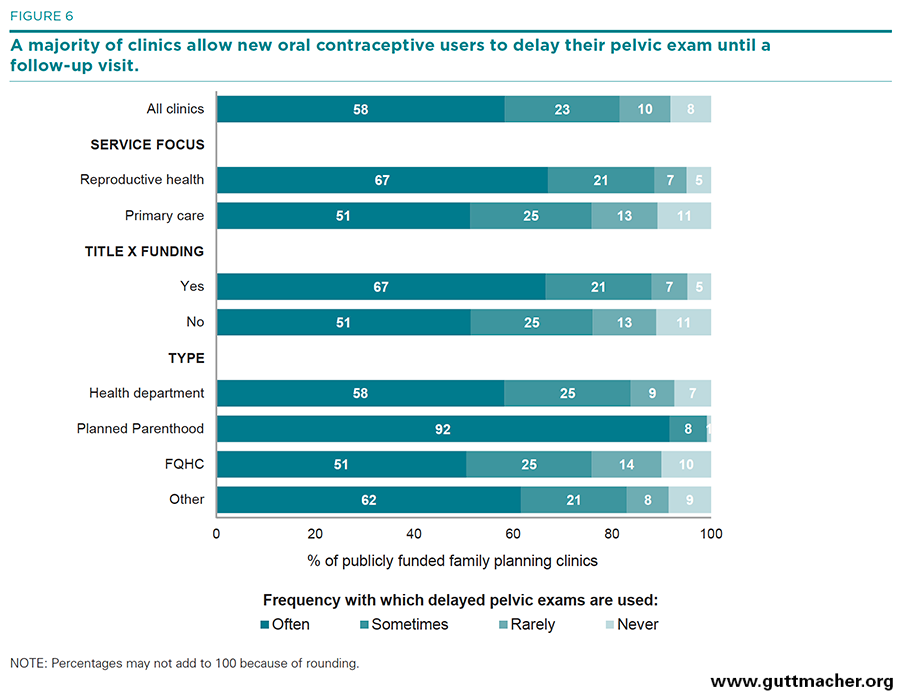
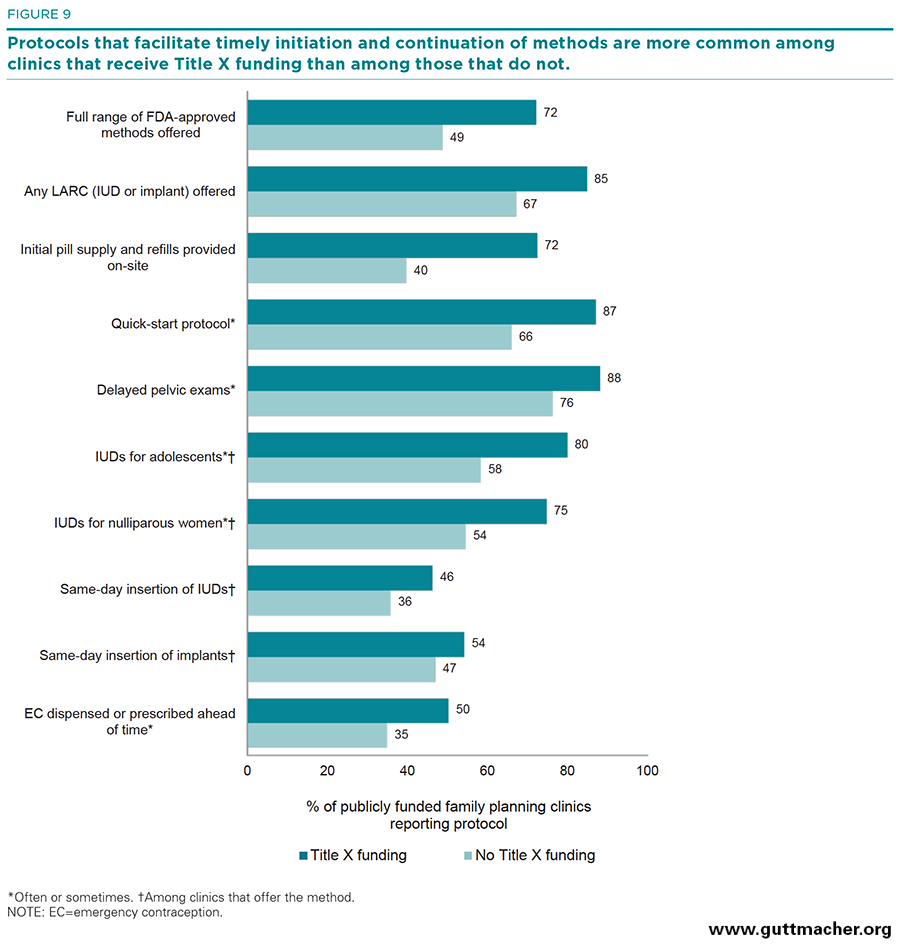
- Along with increased method provision, between 2010 and 2015 clinics were more likely to offer same-day appointments, to have shorter wait times for an appointment, and to have protocols in place that facilitate initiation and continuation of oral contraceptives and LARC methods for women who choose them, including offering “quick-start” and delayed pelvic exam protocols for new oral contraceptive users. Clinics were also more likely to offer noncontraceptive services in 2015, such as primary care services, diabetes screening and mental health screening.
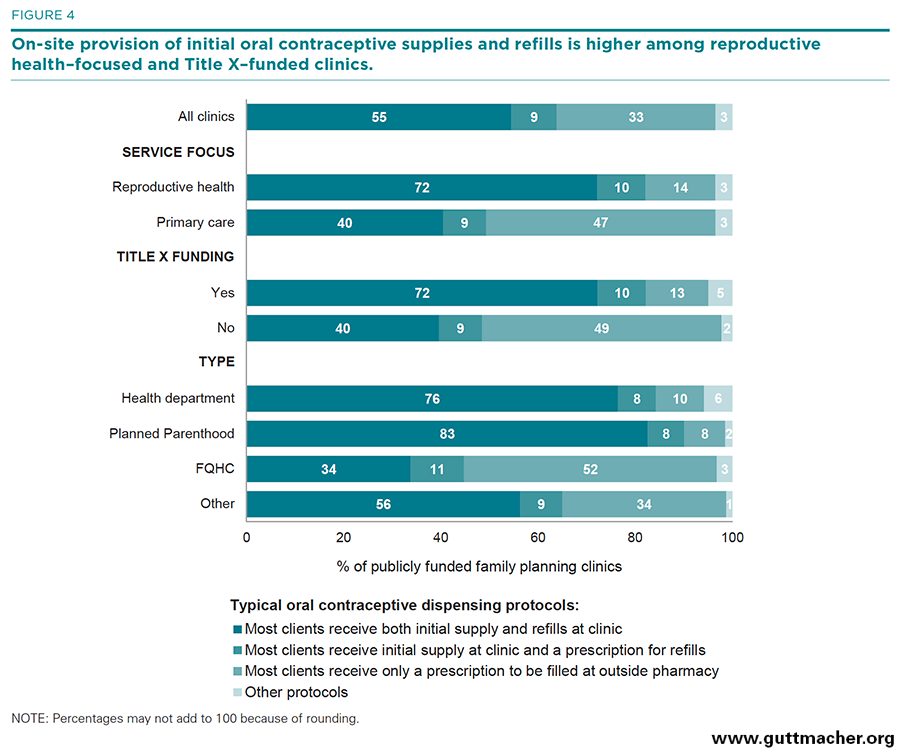
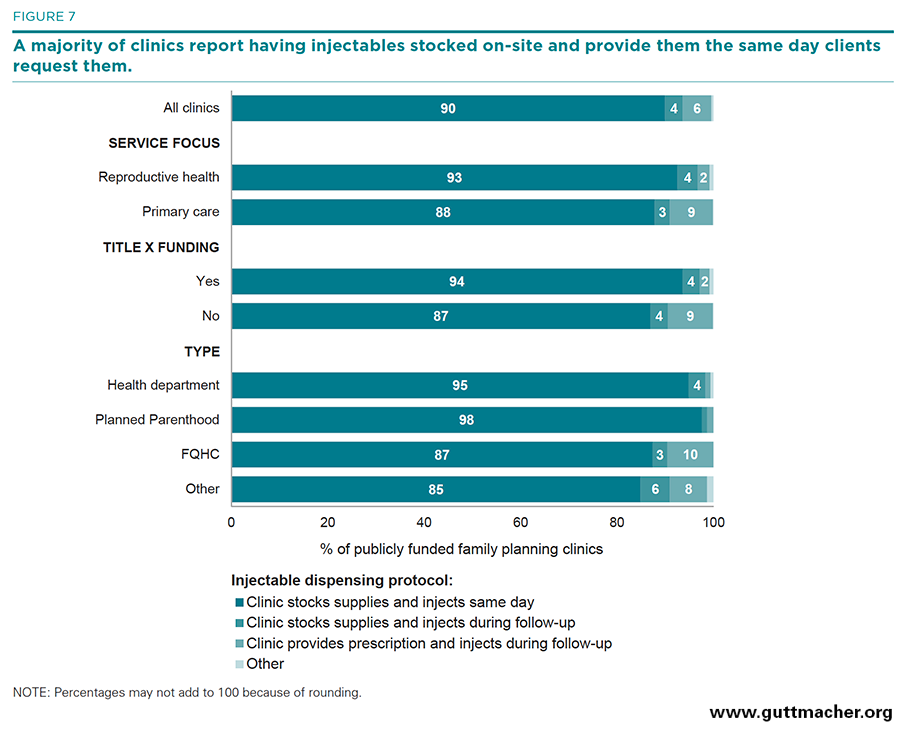
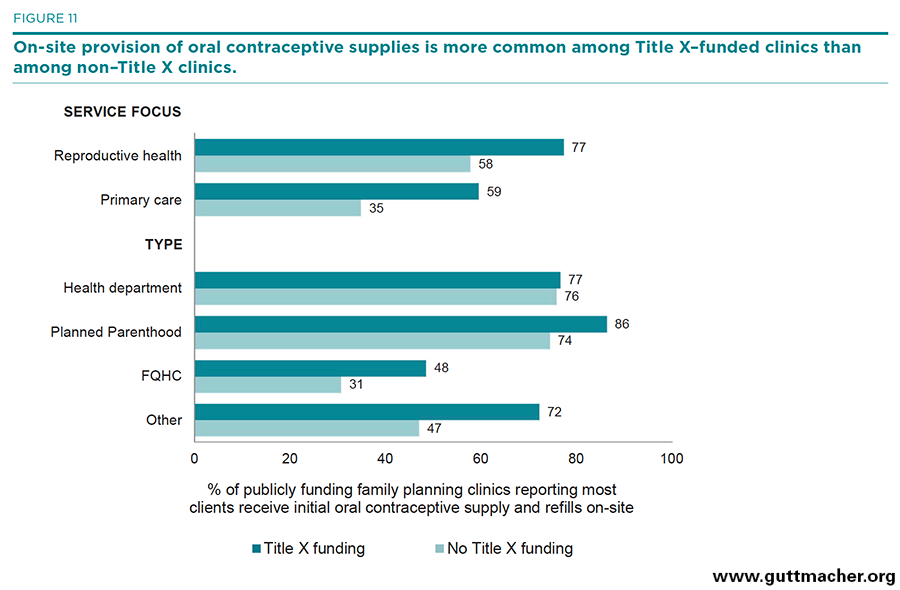
- Clinics that receive at least some funding through the federal Title X program were more likely than clinics that do not receive such funds to offer a wider range of contraceptive methods on-site and to have protocols that facilitate initiation and continuation of oral contraceptives and LARC methods, including dispensing oral contraceptive supplies at the clinic and same-day insertion of IUDs and implants.
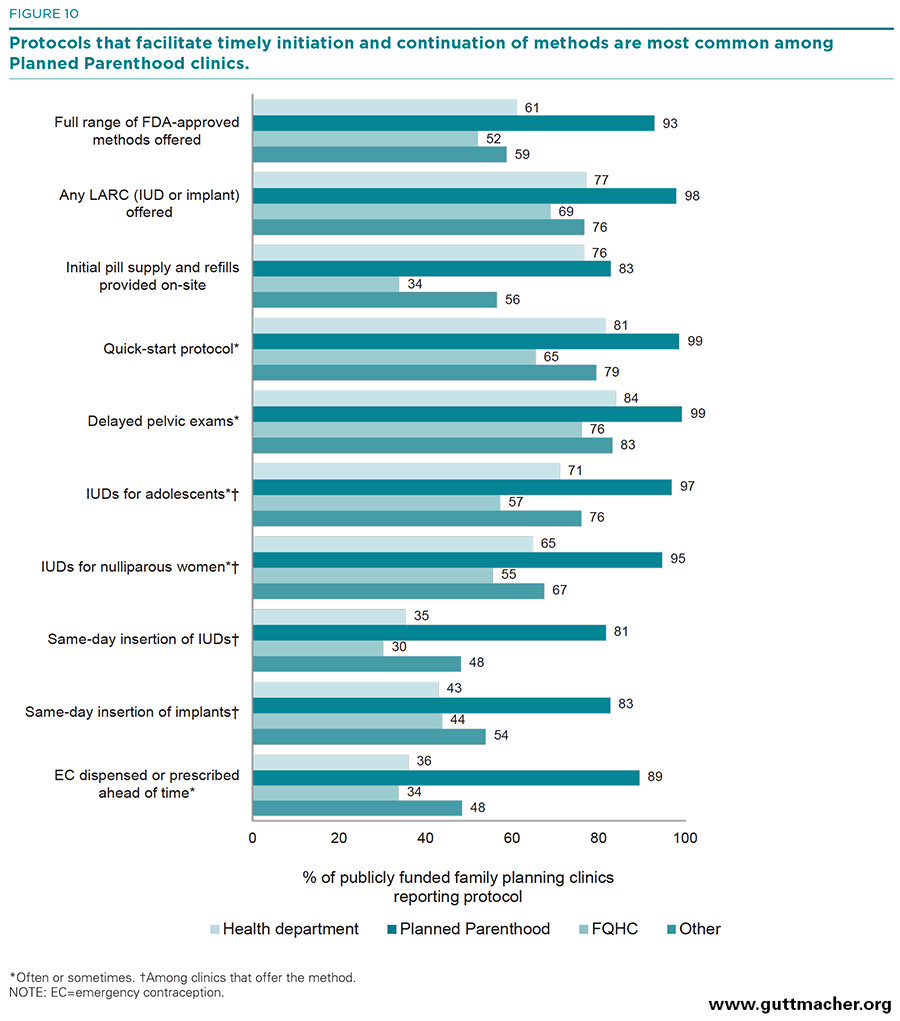
- Planned Parenthood clinics were significantly more likely than any other clinic type to have implemented a variety of protocols that enhance contraceptive method initiation and continuation.
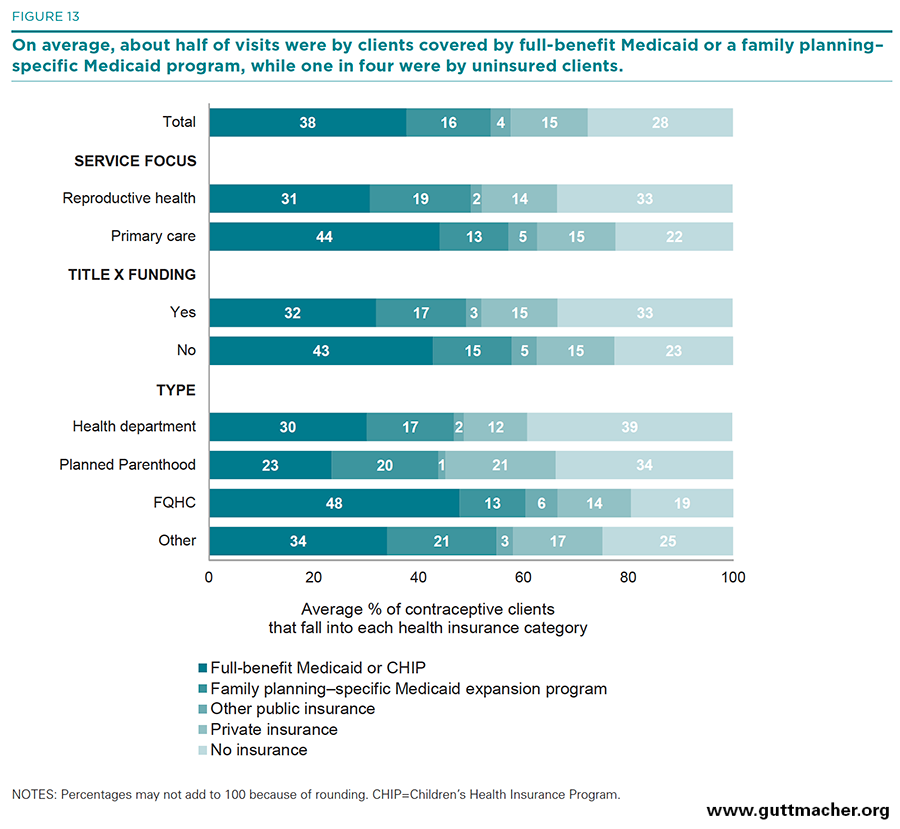
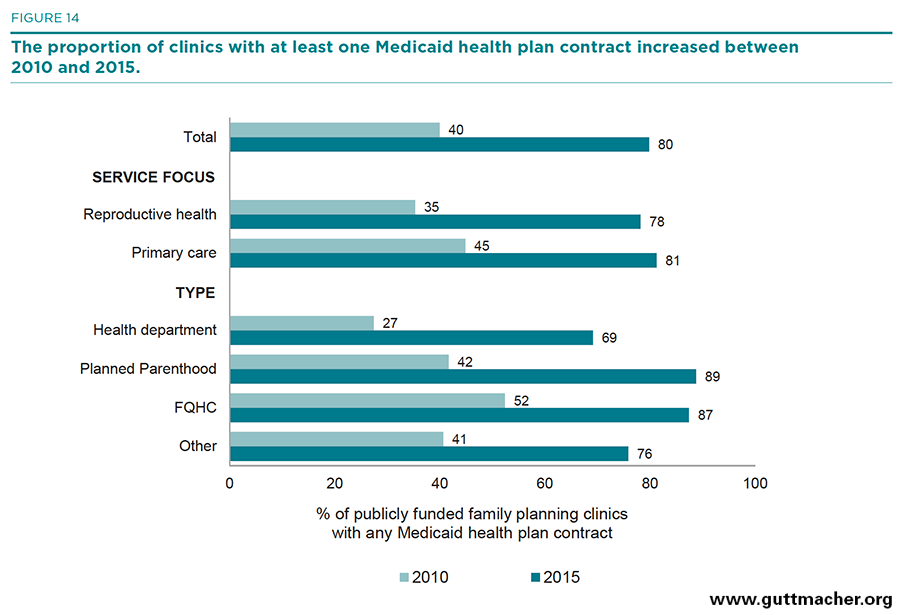
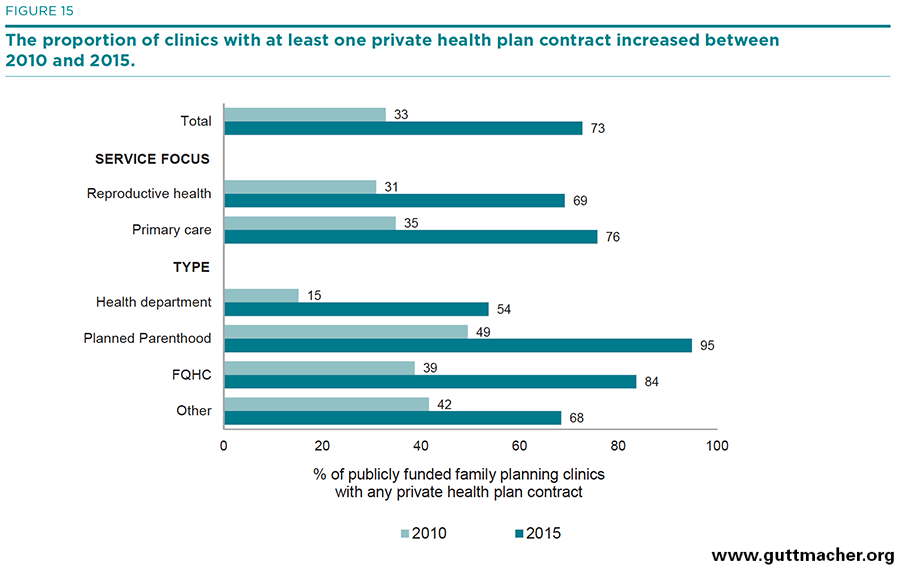
- Between 2010 and 2015, the proportion of clinics reporting contracts with private health plans and with Medicaid at least doubled, indicating a rapid ramping-up of clinics’ ability to function successfully in the new health care marketplace.