This report presents an analysis of policies and curricula on sexuality education in Kenya and their implementation in secondary schools, focusing on key stakeholders and the experiences of principals, teachers and students in three geographically and ethnically diverse counties: Homa Bay, Mombasa and Nairobi.
From Paper to Practice: Sexuality Education Policies and Their Implementation in Kenya

Reproductive rights are under attack. Will you help us fight back with facts?
Key Points
Key Points
- Sexuality education is a key component in a multifaceted approach to address the high need for sexual and reproductive health information and services among adolescents.
- There is support for sexuality education from the Kenyan government, but education-sector policies have largely promoted an abstinence-only approach, which has resulted in a lack of comprehensiveness in the range of topics offered in secondary school curricula.
- There is strong support for teaching sexuality education among principals, teachers and students alike, but the topics that are integrated into compulsory and examinable subjects are limited in scope, and there is little incentive for teachers and students to prioritize them.
- Nearly half (46%) of students were exposed to at least one topic in five key categories related to sexuality education, but only 2% of students reported learning about all of the topics that constitute a comprehensive program as defined by international standards.
- Some messages conveyed to students were reportedly fear-inducing and judgmental or focused on abstinence, emphasizing that sex is dangerous and immoral for young people.
- Students wanted more information on contraceptive methods—including how to use and where to access them—and requested more participatory teaching methods.
- Teachers face significant challenges in the classroom, ranging from lack of time, materials or resources to perceived community opposition, their own discomfort, and lack of knowledge or training on the topics. The improvement, systematizing and scaling up of teacher training are essential to ensure that sexuality education is delivered accurately, appropriately and effectively.
- Coordinated efforts between the government and civil society organizations are urgently needed to develop and implement a comprehensive and age-appropriate sexuality education program in Kenya that is based on internationally recognized standards and the latest evidence on what constitutes a successful program.
Chapter 1: Introduction
Timely provision of accurate and comprehensive information and life skills training regarding sexual and reproductive health and rights (SRHR) is essential for adolescents to achieve sexual health and rights and avoid negative health outcomes.1–3 While sexuality education is just one component in a multifaceted approach to address, and ultimately improve, the sexual and reproductive lives of young people, it provides a structured opportunity for adolescents to gain knowledge and skills, to explore their attitudes and values, and to practice the decision making and other life skills necessary for making healthy informed choices about their sexual lives.2–7 Abstinence-only education programs have shown little evidence of improving sexual and reproductive health (SRH) outcomes.8,9 In contrast, comprehensive sexuality education programs that recognize sexual activity during adolescence as normative behavior, that seek to ensure the safety of such behavior, and that focus on human rights, gender equality and empowerment have demonstrated impact in several areas: improving knowledge, self-confidence and self-esteem; positively changing attitudes and gender and social norms; strengthening decision-making and communication skills and building self-efficacy; and increasing the use of condoms and other contraceptives.3,8–15
Adolescents’ sexual and reproductive health
Addressing the high levels of unprotected sexual activity, STIs (including HIV infection), early pregnancy and abortion among adolescents is a priority for program planners and policymakers in Kenya.16–18 Despite efforts targeting these reproductive health issues, recent studies indicate a persistently high need for SRH information and services, further emphasizing the need for high-quality sexuality education.19–21
Sexual activity
Nationally, more than a third of adolescents (those aged 15–19), whether married or not, have had sexual intercourse (37% of females and 41% of males), and about one-fifth are currently sexually active (Table 1.1). The median age at first intercourse is 18 for females and 17 for males, yet among 15–19-year-olds, 11% and 20% of each gender, respectively, initiated sex before age 15. In the three geographic areas included in the current study, adolescents living in Homa Bay county were more likely to initiate sex at an early age (24% of females and 39% of males) than were those living in Mombasa (6% and 26%, respectively) or Nairobi county (10% and 17%, respectively).
Contraception, unplanned births and abortion
Contraceptive use is relatively low among adolescents in Kenya. Although 96% of all adolescent females have heard of at least one modern method, only 41% of sexually active 15–19-year-olds are currently using any contraceptive method, and 37% are using a modern one.20 The vast majority (93%) of sexually active adolescent females who are unmarried want to avoid pregnancy within the next two years, but 52% have an unmet need for family planning, meaning they either want to postpone their next birth by at least two years or do not want any (additional) children, but are not using a contraceptive method. Among the 12% of adolescent females who are married or in a union, 61% want to avoid a pregnancy, and 23% have an unmet need for family planning. About one-fifth of all adolescents in Kenya have begun childbearing (i.e., have had a live birth or are currently pregnant), and 59% of their births in the past five years were reported as unplanned. There is also evidence that adolescents are particularly vulnerable to severe complications from clandestine unsafe abortions.19 A 2013 study on the incidence of and complications from unsafe abortion in Kenya indicated that 10–19-year-olds accounted for 17% of all women who sought postabortion care in public facilities, and that 74% of the moderate or severe complication cases were among this group, partly because of their use of less-skilled providers.
HIV prevalence and knowledge
HIV infection among adolescents remains a concern in Kenya, despite multiple efforts to reduce its prevalence.22 Nationally, 62% of females and 81% of males aged 15–19 know where to get condoms, but only 49% and 58%, respectively, have comprehensive knowledge of HIV and AIDS.*20 HIV disproportionately affects young women: HIV prevalence among 15–24-year-olds is 4%, compared with 2% among their male counterparts,23,24 and the number of new infections among females aged 10–19 in 2015 was more than double that among males in the same age-group (13,000 vs. 5,100).23
Sexual violence and harmful traditional practices
Among 15–19-year-olds, 7% of females and 3% of males in Kenya have experienced sexual violence, and 4% and 1%, respectively, had the experience by age 15.20 Six percent of adolescents who have ever been pregnant have experienced some form of physical violence during pregnancy. Female genital cutting persists as a traditional practice, despite being outlawed since 2011;25 nationally, 11% of adolescents have undergone this procedure.20
The need for sexuality education in Kenya
As these indicators demonstrate, the contexts in which adolescents in Kenya must navigate their sexual and reproductive lives are complex and, in some cases, vary by region and gender. In recognizing that improving adolescents’ access to high-quality information and services is essential for ameliorating negative health outcomes, key stakeholders in Kenya have proposed policies and programs regarding adolescent SRH, including those related to sexuality education.18 Implementation of new policies, however, has been difficult in the absence of official legislation to enforce them. A major challenge in this effort has been to reconcile rights-based approaches that emphasize adolescents’ right to comprehensive SRH information and services with deeply rooted conservative approaches that stigmatize or denounce certain aspects of SRH education and services, such as improving access to condoms.26,27 The legal and policy environments are discussed in Chapter 3.
Scope of this report
Reviews of policies and curricula pertaining to sexuality education have shown that while many countries have established curricula, little is known about their use in schools—the degree of implementation, the mode and quality of the instruction, the existence of program monitoring and evaluation tools, the adequacy and quality of teacher training, the level of support for or opposition to the subject, and the effectiveness of existing programs in achieving desired knowledge and behavioral outcomes among students.28–33 Small-scale reviews of school-based programs run by nongovernmental organizations (NGOs) have been conducted in Kenya, but there has not been a review of the government’s sexuality education program in schools.34,35
This report provides a snapshot of how sexuality education policies in Kenya are translated into practice in secondary schools, and what students, teachers and principals think about them. Data from official documents, key informant interviews and school-based surveys were used to examine how sexuality education programs in three counties were developed, implemented and experienced. This report presents findings on the development of policies and curricula, including the actors involved and challenges faced; how sexuality education is taught in classrooms; students’ experiences and preferences; support for implementation, including teacher training and school environment factors; sexuality education outside of the classroom; and general opinions about sexuality education among key stakeholders. The information presented is intended to provide the Kenyan government and other stakeholders with a better understanding of sexuality education in its schools, and ultimately to improve the quality and effectiveness of such education for both teachers and students.
Chapter 2: Study Methodology
The study on which this report is based was conducted as part of a multicountry study to assess the implementation of sexuality education in four countries from two regions (Latin America and Africa): Peru, Guatemala, Ghana and Kenya.† In each region, one country was chosen that is at a relatively more advanced implementation stage with its sexuality education program (Peru and Ghana), and another was chosen that is at an earlier stage (Guatemala and Kenya); these selections were based on reviews of policy documents and curricula, program evaluations and other regional reports,30,31,36,37 as well as consultation with stakeholders and research partners. While a major aim of the overall study is to compare all four countries, this report presents findings only for Kenya.
Study objectives
The goal of this study was to provide a robust, comprehensive analysis of policies and curricula regarding sexuality education in Kenya and their implementation in secondary schools, with a focus on three geographically and ethnically diverse counties: Homa Bay, Mombasa and Nairobi. Specific objectives included documenting policies and curricula on sexuality education, describing the implementation of these, assessing the comprehensiveness of the content, examining the opinions and attitudes of students and teachers regarding sexuality education, and providing recommendations to inform the design and implementation of such programs in schools in Kenya and beyond.
Defining comprehensive sexuality education
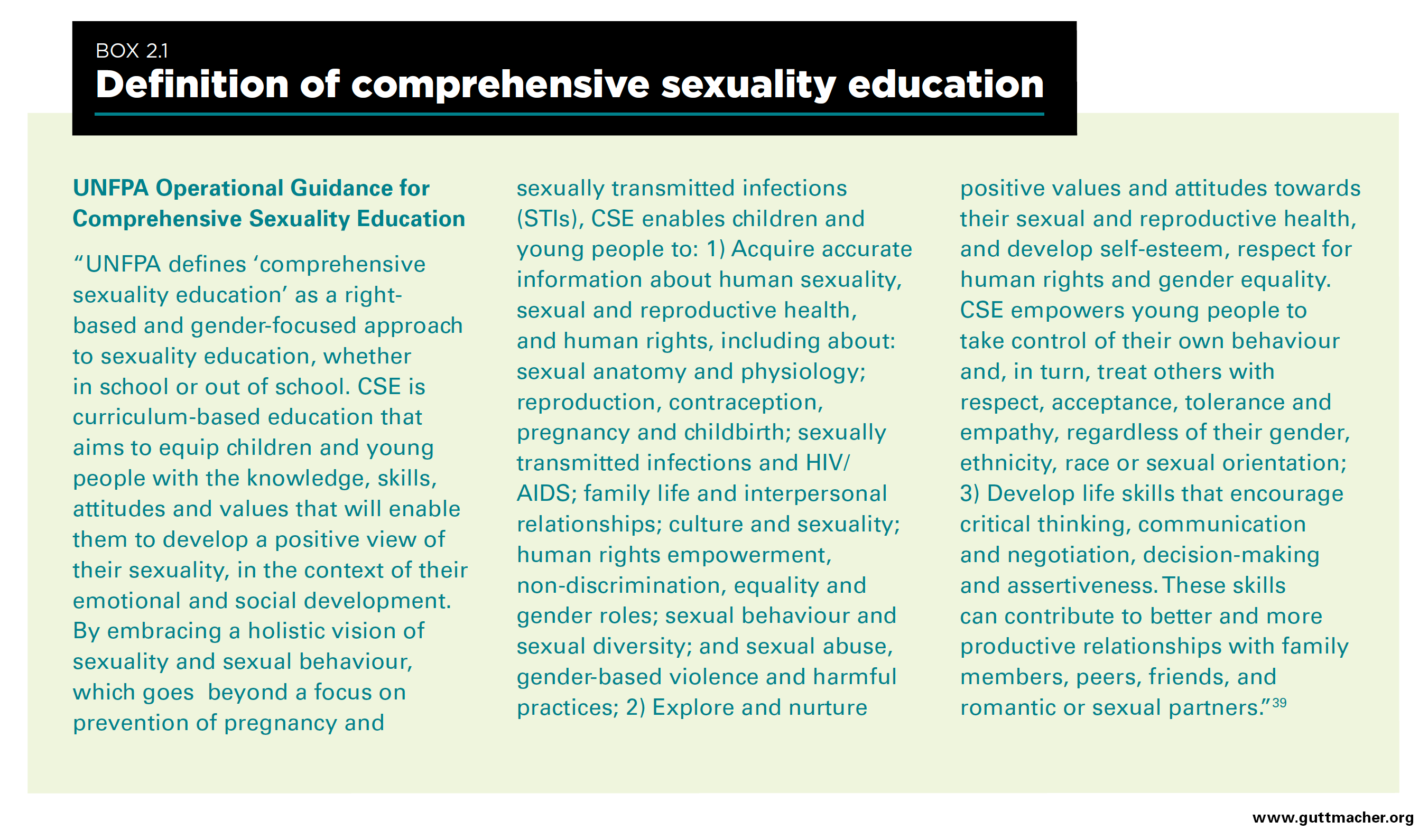
While different definitions of comprehensive sexuality education (CSE) have been developed over time,4–7,38,39 this study used the United Nations Population Fund (UNFPA) definition (Box 2.1). On the basis of the UNFPA definition, this study explored sexuality education according to three dimensions: information and topics covered, values and attitudes nurtured, and life skills developed.
Assessing the comprehensiveness of topics offered
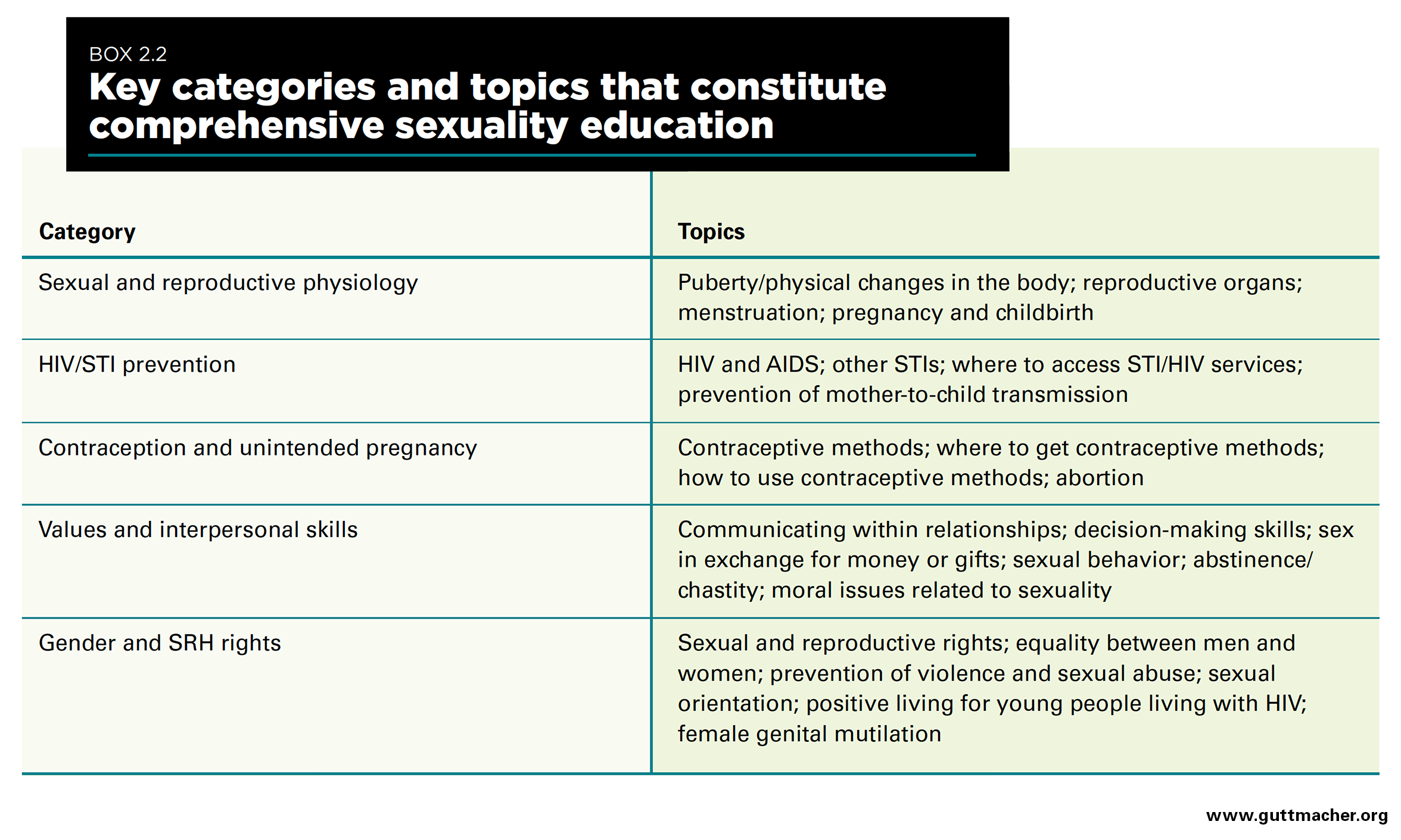
One aim of the study was to measure the comprehensiveness in the range of topics offered. Although the Kenyan government does not claim to be providing comprehensive sexuality education in schools, we assessed the range of topics according to international standards, in order to provide a baseline measure for developing policies or curricula in the future. The topics considered in this study reflect a broad approach that could reasonably be expected in Kenya, given cultural contexts. We did not include topics such as sexual pleasure or desire, which are not culturally appropriate in the country setting. We did include abstinence, as this approach persists in many developing (as well as some developed) countries. Using various international guidelines, we identified five topic categories as key components of a comprehensive program (Box 2.2). The presence or absence of the topics in each category was used to measure comprehensiveness in the range of topics offered. We defined three levels: minimum, adequate and high. If at least one topic in each of the five categories was included, the range met at least a "minimum" level.‡ If nearly all topics (except one at most) in each of the categories were included, the range was considered at least "adequate." The range was deemed to meet a "high" level of comprehensiveness if all topics in each category were included. These levels of comprehensiveness are not mutually exclusive; for example, schools that meet an "adequate" level also meet the "minimum" level, but will be categorized at the highest level achieved.
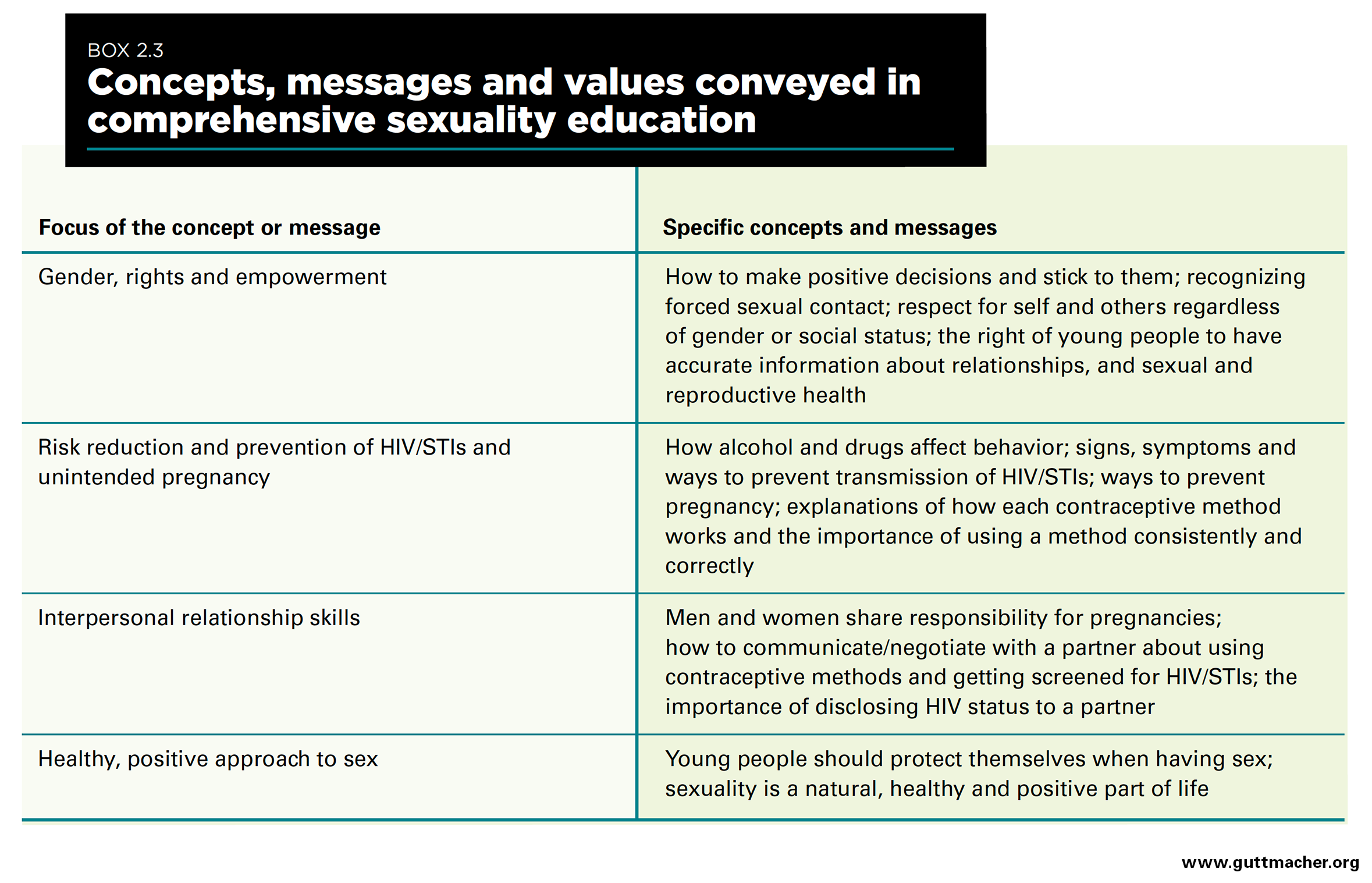
In addition to these topics, our study examined concepts and messages that may be delivered—and the values, attitudes and life skills nurtured—as part of a comprehensive approach to sexuality education (Box 2.3). These elements focus on gender, rights and empowerment, risk-reduction skills, interpersonal relationships and positive views on healthy sexuality. To gain a more nuanced understanding of what is taught in the classroom and the tone in which the teaching is delivered, we assessed, among both students and teachers, the extent to which the concepts and messages were emphasized. We do not, however, include these aspects in our measure of comprehensiveness in the range of topics.
Limitations of the comprehensiveness measure
The measure we developed addresses only the range of topics taught, not other essential components that may determine the comprehensiveness of a sexuality education program, such as integration of youth and community engagement into curriculum development, use of participatory teaching methods, safety of the learning environment, and links to SRH services and other initiatives that address adolescent sexual and reproductive health (ASRH) issues.26,40,41 Moreover, the measure does not assess the depth or manner in which a topic is addressed. For example, our measure assessed whether a school teaches about contraception, but did not capture the accuracy of information, the value judgments conveyed or the time spent teaching about contraception.
Study design
This cross-sectional assessment evaluates the implementation of sexuality education in three counties in Kenya. In addition to reviewing existing documents, the study collected data from three sources.
In-depth interviews with key informants. Informants were asked about their views on current sexuality education policy; opinions about the design, structure, coverage and content of the program; experiences implementing sexuality education in the school system, including how to better support it and challenges faced; perceived sources of support for or opposition to implementation at the national, district and school levels; and monitoring and evaluation frameworks in place.
Survey of secondary school principals and teachers. Researcher-administered surveys elicited interviewees’ responses regarding the content of the curriculum; approach and format of sexuality education in schools; teacher and student assessment methods; teacher training and support; school environment and perceptions of support for or opposition to the subject; and attitudes toward sexuality and SRH issues.
Survey of secondary school students. Self-administered surveys assessed students’ exposure to sexuality education; preferences regarding content, teaching approach and format of the information received; level of support for or opposition to sexuality education in schools; and attitudes toward SRH issues.
Sampling strategy
Key informant interviews
Twenty-five key informants were identified through consultation with a wide range of stakeholders involved in policy making, program implementation or advocacy regarding sexuality education. Informants included Ministry of Education staff involved in the development of policies and curricula related to sexuality education, as well as national stakeholders and individuals with international agencies and NGOs involved in implementation. Also included were individuals working for groups advocating for or opposing the provision of sexuality education in schools, and leaders of community organizations (e.g., youth associations), parent-teacher associations, women’s groups and religious groups.
Survey of schools
Selection of schools. Because the study targeted students aged 15‒17, surveys were conducted in secondary schools.§ Seventy-eight secondary schools were selected across the three counties (Table 2.1); this number was based on a minimum required sample of 2,500 students, and a low-end estimate of 35 eligible students per school, using typical school and grade sizes. The sampling frame was an updated 2014 school list from the Kenya Ministry of Education.** For each county, the sample was stratified by school type (public or private) and coeducational status (mixed gender, females only or males only) to ensure a representative sample.†† We did not analyze the data for all of these strata: This report examines differences by school type but not by coeducational status, owing to the small number of single-gender schools in our sample. Although schools were sampled from three counties representing a geographically and ethnically diverse range of areas, the findings presented in this report should not be interpreted to be nationally representative.
Of the 78 targeted schools, 18 did not grant permission to conduct surveys and were therefore dropped from the sample and replaced. Sixteen of these were private schools in Nairobi and Mombasa, many of which were highly selective or international schools; they declined because of lengthy internal procedures to obtain approval, rather than an objection to the study itself.
Selection of principals and teachers. All principals from selected schools were eligible. In five schools, principals were unable to make time for the survey; therefore, only 73 schools are represented for school-level indicators that rely on information from principals. Teachers were selected on the basis of their involvement in teaching sexuality education topics to students in Form 2 or 3 (i.e., the second and third years of secondary school). Since sexuality education is integrated into life skills, biology and religious education, teachers of these subjects were targeted in each sampled school. These teachers were identified through consultation with the school principal, and up to three teachers per school were selected on the basis of availability on the day of the survey and an aim to cover the range of subjects in which sexuality education topics are taught. In one school, no teachers were available, so only 77 schools are represented for school-level indicators that rely on teacher-level data.
Selection of students. All students in Forms 2 and 3 and aged 15–17 were eligible for sampling in each school. These students were selected because they were likely to have been exposed to at least one year of sexuality education in secondary school and could therefore provide the information we sought to collect. Although this age range was targeted, students aged 13–14 and those older than 17 who were in Form 2 or 3 were not excluded from participating. Five percent of students who participated were younger than 15, and 7% were older than 17. Updated data on the number of students in these forms were obtained from each school prior to sampling. To ensure equal representation of each school within its county, the number of sampled students per school was proportionate to school size. To minimize potential bias, all eligible students in Forms 2 and 3 at each school were gathered in a room and a ballot box was used to randomly select the desired sample of students.
Instrument development and data collection
The interview guide and questionnaires used in this study were developed by an international team of researchers; they drew from multiple instruments that have been used to assess aspects of sexuality education both in and out of school.1–3,40,42–46 Discussions were held with representatives from the Kenya Ministry of Education, the Kenya Institute of Curriculum Development, the United Nations Educational, Scientific and Cultural Organization (UNESCO), the Population Council and various local organizations to gather necessary data or information that was used to refine the tools and make them country-specific.
The study protocol was approved by the Guttmacher Institute’s institutional review board and the AMREF Ethics and Scientific Review Committee. A research permit was obtained from the National Commission for Science, Technology and Innovation in Kenya. Authorization letters to enter schools were obtained from county education officials and school authorities in the respective study areas. The principals of all sampled schools were contacted by phone to introduce the study and solicit participation. Following this initial contact, letters were mailed to schools announcing the date that the research team would visit to conduct the surveys. Informed consent and assent were sought from all participants. To maintain students’ anonymity, neither principals nor teachers knew which students completed the survey. All information provided by respondents was treated as strictly confidential, and access was denied to anyone outside of the research team. Quotations from key informants have been anonymized.
Key informant in-person interviews were conducted between November 2014 and August 2015. All interviews were done in English, audio recorded (subject to interviewees’ informed consent) and transcribed. Surveys of principals, teachers and students were conducted between February and July 2015.‡‡ Questionnaires were in English in Nairobi and Homa Bay, and in Kiswahili in Mombasa.
Data management and analysis
Qualitative data were examined using thematic and content analysis in NVivo. Quantitative data were entered into CSPro, cleaned and checked for inconsistencies, and transferred into Stata 13.1 for analysis. Descriptive analyses were conducted by type of school (public or private) for each county. To ensure that all estimates were representative at the county level, sample weights were applied to account for the different probabilities of a school, student, teacher or principal being selected to participate. We provide the unweighted sample sizes in the tables.
We present county-level data in tables at the end of the report, but in the text we present summary measures of the three counties combined. Figures are used to depict key findings, and all data provided in the figures also appear in the tables. We note specific differences between counties, and by school type and gender, only when those differences are statistically significant and have programmatic or policy relevance. We report differences by gender for measures related to students’ perceptions of school safety and out-of-school experiences with sexuality education. All significance tests account for clustering at the student and teacher levels to ensure correct variance estimates. Pearson’s chi-square tests were used to detect differences in proportions and percentage distributions among counties, between public and private schools, and between females and males. When "other" response categories accounted for more than 5% of responses for a particular variable, these responses were analyzed and recoded into existing or new categories.
For some school-level indicators, especially those related to policies or program structure, we considered principals’ responses to be representative of the entire school. However, for most school-level indicators, we relied on teachers’ and students’ responses, as they are more familiar with classroom practice. For questions asked of teachers, but presented at the school level, we classified a school response as "yes" if one or more teachers responded affirmatively; if one teacher in a school was teaching an aspect of sexuality education, then we considered it offered in the school to some capacity. For questions asked of students and presented at the school level, we classified a school response as "yes" if at least 20% of students responded affirmatively to a particular question. We did not choose a higher cutoff because we wanted to ensure that a school was counted as offering a topic even if only a few students reported it, since only one of the grades surveyed may have covered it, or not all students may have taken that particular class. We required at least 20% of students because—while the average number of students per school in our sample was 32—some schools were very small and some indicators were based on a subsample of students. Capturing responses from at least 20% of students ensured that we were basing our estimates on the responses of more than one student per school in the very small schools.
In sections that present both teacher-level and student-level data, the teachers’ responses cannot be directly compared to those of students, even though in most cases we asked teachers and students similar questions. Topics related to sexuality education are included in different subjects and taught differently by multiple teachers, and we did not track which students were taught by which teachers. Rather, the teachers’ responses reveal the overall experience of teachers who cover the various topics, and the students’ perspectives show the overall experience among the student body.
Throughout the report, we present students’ and teachers’ experiences as they occurred in schools during normal school hours. Students are also exposed to sexuality education through a number of channels outside of the formal school setting, such as peer educators, media, parents and extracurricular activities (see Chapter 6). While such exposure can influence students’ attitudes and knowledge regarding sexuality education, we do not expect it to influence their responses to school-based questions nor affect our assessment of classroom practice. Summaries of key findings are presented at the ends of Chapters 3–7.
Response rates and characteristics of samples
Nearly all selected key informants participated in the study. Two were replaced by other respondents in the same organization because of availability at the time of the scheduled interview. A total of 78 schools were sampled, and survey response rates were relatively high for all types of respondents. For details on response rates, see Table 2.2; for details on characteristics of survey respondents, see Table 2.3 for principals, Table 2.4 for teachers and Table 2.5 for students.
Chapter 3: Sexuality Education in Kenya
This chapter describes the policy and legal environment regarding sexuality education in Kenya, the actors involved in curriculum development, the structure and content of the sexuality education program, and challenges to program development and implementation, and offers commentary on program comprehensiveness. This information is drawn from a desk review of policy documents and syllabi currently used in secondary schools, previous curriculum reviews and key informant interviews.
The legal and policy environment
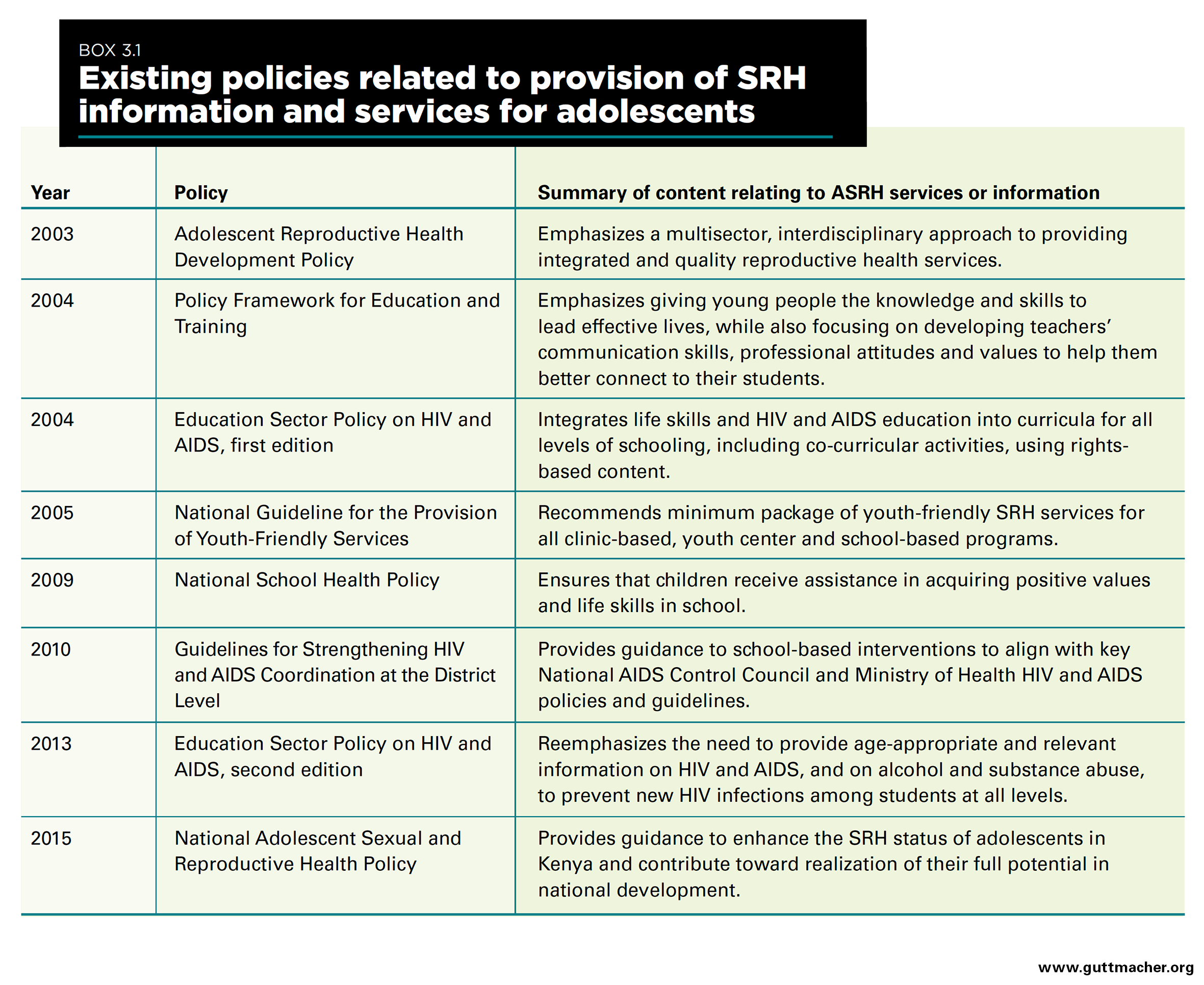
The provision of SRH information and services to adolescents in Kenya is supported by various health and education policies (Box 3.1). The provision of sexuality education is supported by the 2004 Policy Framework for Education and Training and the 2004 and 2013 Education Sector Policy on HIV and AIDS. Existing educational policies, however, still emphasize life skills and HIV education, and thus are limited in scope. Ministries of Education from the East and Southern Africa region, including Kenya, signed a declaration in 2013 in which they committed to scaling up comprehensive rights-based sexuality education beginning in primary school.28 This declaration built on a 10-country review of sexuality education curricula by the Population Council in 2012.31
Actors involved in curriculum development
The development of the sexuality education curriculum is the mandate of the Ministry of Education through the Kenya Institute of Curriculum Development.§§ The development process, which is conducted in multiple steps starting with a needs assessment, involves input from various entities, including government ministries, religious groups, local and international NGOs, and local communities. Several NGOs in Kenya have developed their own materials, but these cannot be used by teachers in schools (public or private) without prior review and approval from the Institute and the Ministry of Education.
According to the key informants, the actors involved in the development of the curriculum and policies include teachers, government departments and ministries, United Nations bodies, civil society organizations, activists and professional groups, but not adolescents themselves. The exclusion of the views and experiences of students—the intended beneficiaries—is an issue that commonly arises in the development and design of sexuality education programs, and is not unique to Kenya.18
Curriculum content and structure
Kenya’s life skills education curriculum was originally developed by the Ministry of Education in 200247 and revised in 200848 (Box 3.2). The new syllabus promotes general skills for day-to-day living, such as self-appreciation, improving interpersonal relationships, acquiring decision-making skills, respecting other people’s rights and coping with stress and emotions.
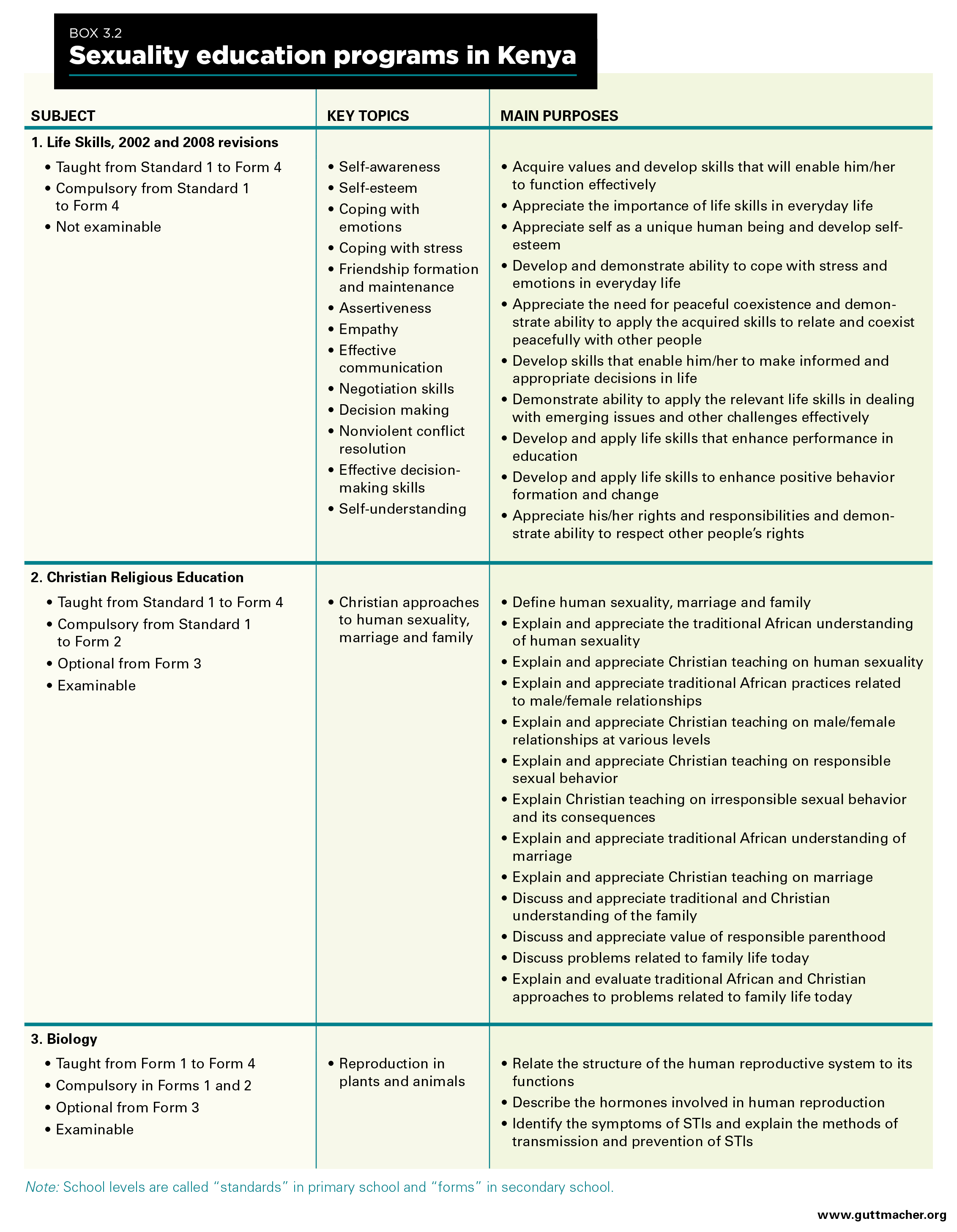
Sexuality education, as defined in this study, is not explicitly included as a stand-alone, examinable subject in the Kenya national curriculum. Instead, some topics related to SRH education have been included in different subjects, such as life skills (arguably the most comprehensive of the three), Christian religious education and biology. Box 3.2 offers a detailed description of key topics included in each of these subjects, the grades in which they are taught and whether the subjects are compulsory or examinable. The latter point is relevant to curriculum implementation because more emphasis is given to examinable subjects49 (i.e., those that are academically scored), and teachers prefer teaching those subjects. Religious education and biology are examinable, while life skills is not.
Sexuality education yes, but how comprehensive?
In 2011, UNESCO and UNFPA conducted a review of sexuality education curricula in Kenya and nine other Eastern and Southern African countries to assess their content, quality and delivery methods.***31 Overall, key areas of strength in Kenya, as well as in the other countries, included age-appropriate content; reasonable coverage of communication skills, broadly focusing on refusal skills and risk avoidance; and an increasing focus on gender. The curricula were considered weak in a number of areas: They emphasized abstinence; lacked adequate basic information on contraceptives, condoms, sex and sexual health; excluded key topics such as reproduction, STIs, abortion, access to condoms and sexual health services; and omitted other social and contextual aspects, such as harassment and parental monitoring.
The review found that the curriculum in Kenya used prescriptive and fear-based teaching methods and lacked depth in its overall content, which did not foster enough critical thinking for students to better understand sexuality and reproductive health. Moreover, the curriculum lacked basic information on HIV prevention (e.g., using condoms), and there was a weak focus on gender and human rights issues, such as the rights of people living with HIV. Topics such as forced sex, gender-based violence and intimate partner violence were largely ignored. The review emphasized that the information provided to students was insufficient to help in reducing the risk of HIV, STIs and unintended pregnancy.
Nearly all key informants agreed that sexuality education offered in secondary schools was not comprehensive. The curriculum is focused on biology and excludes topics related to SRHR, and the approach was described as purely academic with little attention to improving students’ practical skills. There were differences in opinion among respondents regarding what content should be covered in a "comprehensive" program. Several noted that sexuality education must include information on contraceptives and pregnancy prevention, and take a holistic approach to education to provide adolescents with the requisite skills to transition to adulthood. Others insisted that topics such as abortion, contraceptives and sexual orientation should be excluded from sexuality education initiatives targeting adolescents. Respondents who held a more restrictive viewpoint cited religious and cultural inhibitions about discussing sexual matters with students, and some stakeholders opposed inclusion of topics related to contraceptives because such information was deemed to encourage teenage sex. The evidence base, however, shows that making the link between improved access to contraceptives and increased sexual activity among adolescents is an incorrect belief.2,5
A national NGO respondent opined that Kenya’s curriculum is "obsolete" and may not be responsive to emerging issues in society. Although the process of reforming the curriculum is under way and would incorporate views from a wide range of stakeholders, it is a lengthy process and expected changes may not be included for years. In the meantime, as mentioned by a respondent from the United Nations, other stakeholders, such as civil society organizations, have stepped in to complement the Ministry of Education efforts by providing extracurricular activities for students in an effort to create awareness about sexuality issues that may not be covered in the current curriculum.
Challenges to program development and implementation
A number of barriers to effective implementation of sexuality education in schools were identified by key informants: opposition from religious and conservative groups, cultural silence regarding sexuality, lack of teachers well-trained in sexuality education, poorly supported schools, absence of a clear framework for translating policies into practice, and weak regulation and supervision of the implementation of existing policies. These drawbacks culminate in the failure and inability of many schools to offer CSE to their students, and result in a substantial gap between policy and practice.
Another notable challenge identified by key informants is the centralization of education in Kenya. The majority noted that in theory, centralization ensures national investments in teacher training and curriculum development, wider coverage of programs and continuity of content delivered in schools across the country. However, it was also noted that a decentralized approach to school-based sexuality education would allow for programs to be adapted to different contexts, would reduce bureaucratic delays and barriers, and would encourage counties to prioritize the needs of adolescents and young people. Key informants elaborated on several of these issues:
"I also think [the centralization of education] is positive and negative; positive in the sense that if you want to influence the policy, it is much easier, and once you get it approved, it will be easy to scale it down. And I would also support the county government where it is decentralized, whereby you see every county has a different situation for those young people. Then it would be much easier to approach each county according to the situation of the people there and convince them."
—Respondent from an international NGO
"[The curriculum] will deliver the national objectives in education, but not really a context-specific, contextualized education.... For instance, when you look at issues that you might need to address, assuming you want to address issues in West Pokot or Kajiado, you might want to have content which is not only SRH-specific, but [is specific to female genital mutilation and gender-based violence, issues that] might be irrelevant in Makueni or some other areas where they don’t practice [female genital mutilation]. You might not want to use the same methodology to talk about HIV, or even the same emphasis when you are doing it in Kisumu—[or] areas with high HIV prevalence—compared to some other areas which are considered to have low prevalence rates."
—Respondent from a national NGO
Summary of findings
- The provision of sexuality education to adolescents nationally is supported by several national policies and guidelines, although these focus on life skills and HIV and lack comprehensiveness. In 2013, the Kenyan government signed a declaration in which they committed to scaling up comprehensive rights-based sexuality education beginning in primary school.
- Progress toward reaching this goal has been slow, in part because of differences in opinions and agendas between key stakeholders—such as parents, religious groups, the Ministry of Education, NGOs and students—and because of a lack of collaboration among interested parties in the development of sexuality education policies and curricula.
- Historically, the comprehensiveness of policies and curricula has fallen short in comparison with international standards, largely owing to challenges posed by conservative societal norms, cultural sensitivities and education-sector policies that primarily promote abstinence.
- Published reviews and interviews with key informants cited the use of fear-based or negative frames to introduce sexuality; a weak focus on gender and human rights; missing information in a number of key topic areas, including contraceptive methods, sexuality and abortion; and lack of responsiveness to emerging societal issues.
- Sexuality education is not a stand-alone subject in the national curriculum. Instead, specific topics are taught in other subjects, such as life skills, Christian religious education and biology. Life skills is the most comprehensive of these subject areas; it is compulsory but not examinable, which is problematic because most teachers place more importance on teaching academically scored subjects.
- Key informants identified several challenges to the effective implementation of sexuality education, including lack of well-trained teachers, poorly resourced schools, absence of a clear framework for translating policy into practice, and weak regulation and supervision of the implementation of current policies.
- The education system in Kenya is centralized, which ensures government commitment, wide coverage of programs and continuity of content across counties, but some key informants suggested that the design and implementation of sexuality education could benefit from a decentralized approach that would focus on context-specific content, reduce bureaucracy and encourage local stakeholders to prioritize adolescent sexual and reproductive health.
Chapter 4: Sexuality Education in the Classroom
Several aspects of sexuality education contribute to its effectiveness, including its placement in the curriculum, pedagogical approach, timing of delivery, and the comprehensiveness of the skills and information it imparts. This chapter presents findings on the implementation of sexuality education in schools, relying on the surveys with principals, teachers and students and on key informant interviews to describe the organization of the program, the timing and format of teaching, curriculum content, teaching methods, class environment, and monitoring and evaluation systems in place.
Organization, timing and format
While all surveyed schools teach topics related to sexuality education as part of the national curriculum, 43% also teach the topics as an extracurricular activity (Table 4.1). These activities include drama, clubs, sports and music. The sexuality education program is run by the government in 56% of schools and by NGOs in 24%. Three-fourths of schools involve peer educators to teach sexuality education; this is more common in public (92%) than in private (61%) schools.
According to teachers, most schools in Mombasa (86%) and Homa Bay (95%) counties dedicated six or more hours per term in Form 2 to topics related to sexuality education, while in Nairobi, only 39% of schools did so (Figure 4.1).††† The hours spent in Form 3 also varied by county: Ninety-two percent of schools in Mombasa, 88% in Homa Bay and 65% in Nairobi dedicated six or more hours per term. Some 67% of students believed that more time should be dedicated to such topics in school (not shown). Among students in coeducational schools who had been exposed to sexuality education, 46% reported that all topics were taught to males and females together, 45% reported that some were taught together and some separately, and 9% said all were taught separately (Table 4.2). There were differences in teaching preferences by gender: A higher proportion of males than of females preferred to have all topics taught together (58% vs. 44%).
While data for this study are from the secondary school level, primary school—where students are usually between seven and 14 years old—is an important entry point to begin addressing topics related to appropriate touching, SRH and gender equality.3 Exposing students to sexuality education in primary school is also advantageous given the high levels of enrollment in primary school compared with secondary school. In 2014, some 86% of females and males were enrolled in primary school, whereas only 33% were attending secondary school.20
The vast majority of students in our study were first exposed to topics related to sexuality education in primary school (96%), while 4% were first exposed in junior high school. The majority of students (65%) began sexuality education in Standard 6 (on average, students in this standard are 12 years old), and 85% of students had received teaching on sexuality education by the time they completed that year. One-fourth (26%) of the students in our sample (mostly aged 15–17) had already had sex—42% of males and 15% of females (see Table 2.5). While many had likely received some school-based sexuality education prior to initiating sexual activity, the information provided in primary school is limited to very basic knowledge of biology and physical changes in the body, and would not have exposed students to information on safe sex.
Most students who reported first exposure to sexuality education in primary school were satisfied with the timing (65%), but 31% said they would have liked to have learned about the topics earlier. As expected, the majority of students learned about sexuality education in life skills (78%) and biology classes (69%; Figure 4.2).
Content of curricula
Topics offered
Teacher perspectives. According to teachers, the topics of HIV and AIDS, other STIs and abstinence are covered in all sampled schools in the three counties (Table 4.3).‡‡‡ Most schools covered contraceptive methods (95%), including how to use them (87%) and where to get them (86%). All other topics were taught in nearly all schools (91–99%). Public schools were more likely than private ones to cover all topics in the values and interpersonal skills category (93% vs. 76%).
On the basis of our methodology described in Chapter 2, the comprehensiveness of the range of topics taught was deemed at least "minimum" from the teachers’ perspectives in 99% of schools, at least "adequate" in 84% of schools and "high" in 76% of schools (Figure 4.3). There were no significant differences by school type or county.
Student perspectives. While we cannot directly compare student and teacher responses, student perspectives on sexuality education topics taught in their classes tell a slightly different story. The topics that students reported most commonly learning about were HIV and AIDS (92%), reproductive organs (88%), puberty and physical changes in the body (87%), abstinence (84%) and other STIs (80%; Table 4.4; Figure 4.4). About four in 10 students reported learning about equality between men and women (43%), abortion (40%), sexual orientation (39%), sexual and reproductive rights (37%) or communicating within relationships (37%). Very few students (20%) reported learning about contraceptive methods; 13% learned how to use contraceptive methods, and 15% learned where to get them, but more than 60% said they would like to learn more about these topics (Table 4.5). Three of the five topics with the largest gap between the proportion of students who reported learning about it and the proportion who wanted to learn more were related to contraceptive methods; the other two topics were female genital mutilation and sexual and reproductive rights (Figure 4.5).
Findings on students’ exposure to topics are particularly striking. Forty-seven percent of students learned about all topics in sexual and reproductive physiology, and students in public schools reported greater exposure than did those in private schools (52% vs. 40%). Forty-one percent of students learned about all topics related to prevention of HIV and other STIs; again, public school students reported more exposure than did students attending private schools (45% vs. 36%), and there were significant differences by county. Only 14% of students learned about all topics regarding values and interpersonal skills, 8% learned about all topics related to gender and SRH rights, and 7% learned about all contraception and unintended pregnancy topics; significant differences were seen between counties for the values and contraception categories (Figure 4.6).
According to students’ reports, the comprehensiveness of the range of topics appeared to meet at least the "minimum" for only 46% of students; it was at least "adequate" for 5%, and was "high" for a mere 2%; the remaining 54% of students did not even learn about one topic in each category (Figure 4.7). While teacher and student responses are not directly comparable because we do not know which teachers taught which students, or in what grades teachers were covering particular topics, it is nonetheless notable that the comprehensiveness of topics covered from the student perspective was much lower than the level reported by teachers. Although some students may underreport what they have learned in an effort to make the case for needing more sexuality education, it is equally likely that they might overreport topics covered in an effort to impress the fieldworkers or prove that they have been attending class and paying attention. These two potential biases would cancel each other out. Teachers, on the other hand, may have an incentive to overreport the number of topics they are teaching if they believe these topics are part of the curriculum and that they should be taught. Although the higher comprehensiveness reported by teachers may be partly due to teachers covering some topics in grades that students have not yet reached, this is unlikely to explain the large discrepancy.
Concepts and messages conveyed
Teacher perspectives. The information provided by teachers confirmed that the messages most of them delivered on sexuality education were focused on abstinence, and this approach set the tone for what students were learning (Table 4.6). The majority of teachers reported very strongly emphasizing that having sexual relationships is dangerous (59%) or immoral (58%) for young people. Teachers were more likely to strongly express the latter sentiment in Mombasa (81%) than in Nairobi or Homa Bay (52% and 67%, respectively). A high proportion of teachers also reported that they very strongly emphasized that young people should avoid having sex before they are married (64%), and this proportion was higher in Mombasa (87%) and Homa Bay (82%) than in Nairobi (58%). In all three counties, two-thirds of teachers very strongly emphasized that abortion is immoral. About half reported that they relayed a very strong message that homosexuality is unnatural, as did 61% of teachers in Mombasa. In contrast, only 34% of teachers reported that they very strongly conveyed the message that young people should protect themselves when they have sex by using condoms. While a majority of teachers in Mombasa and Homa Bay (78% and 74%, respectively) reported strongly emphasizing that young people have the right to know everything about relationships and SRH, only 43% of Nairobi teachers did so. Ninety-one percent of teachers said they covered abstinence, while 83% taught about contraceptive methods (Table 4.7); nearly all taught about condoms (98%), and 61% discussed oral contraceptive pills (Figure 4.8).
While most teachers reported covering contraceptives, the nature of the information varied. A number of messages related to the effectiveness of contraceptives in preventing infection with STIs or HIV and avoiding pregnancy were conveyed. Notably, 21% of teachers who taught about contraceptives emphasized in their classes that they are not effective in preventing pregnancy (Figure 4.9). Fifty-eight percent of teachers who taught about condoms emphasized that condoms alone are not effective in preventing pregnancy (Figure 4.10), while 27% conveyed to students that condoms are not effective in preventing STIs or HIV (Figure 4.11). Finally, 71% of teachers who covered abstinence told students that it is the best or only way to prevent pregnancy and STIs (Figure 4.12).
Student perspectives. While a major aim of sexuality education is to impart the practical skills and knowledge needed for adolescents to safely navigate their sexual and reproductive lives, a minority of students reported being taught practical skills, such as how to talk to a partner about getting tested for HIV (38%), how to recognize forced sexual contact (36%), what to do if a female gets pregnant or a male gets a female pregnant (25%), and how to communicate with a partner about using contraceptive methods, including condoms (22%; Table 4.8).
Comprehensive sexuality education programs seek to teach adolescents to exercise their sexual and reproductive rights safely and responsibly by recognizing that sexual activity at their age is normative. Most students surveyed, however, reported a fear-based and prescriptive tone in the messages they received. Three-fourths reported that their teachers very strongly emphasized that they should not have sex before marriage and that having sex is dangerous for young people. Fewer than half of all students reported that the message to avoid having sex, but to use condoms if they do, was very strongly conveyed. For all of these messages, there were significant student reporting differences among the counties, and for the first two messages, differences were also observed between students attending public versus private schools.
Teaching methods
The use of nonformal teaching methods that involve students as active participants—such as group learning, peer engagement and learner-centered methodologies that aim to build students’ values and critical thinking skills—is increasingly being recognized for the positive influence on learning and education broadly, suggesting that reliance on lectures alone may be insufficient to effectively impart knowledge in a classroom.3 While most teachers in the schools surveyed used lectures or talks (87%), more than half also used small-group discussions (81%), charts and drawings (71%), and creative, participatory learning activities, such as role playing, theater, debates, art projects, dance, poetry and storytelling (69%; Table 4.9). However, only 44% of students reported having participated in small-group discussions, and only 13% reported having learned through use of charts and drawings (Table 4.10). Interestingly, while most students wanted to engage in creative, participatory learning activities (78%), students also expressed interest in activities that were less common in the classroom, such as use of audio-visual materials (55%) and the Internet or social media (41%). Greater proportions of students in Homa Bay county than in Nairobi or Mombasa county had engaged in many of the activities, particularly participatory learning and small-group discussions; students’ preferences for classroom activities followed similar patterns.
Regarding the use of classroom teaching aids, 81% of teachers reported using written materials, 62% used charts, 24% used other audio-visual materials and 8% employed demonstration kits (Table 4.11). Fewer than 10% of teachers showed contraceptive methods to students to demonstrate how they work. Twenty-seven percent of teachers reported showing the proper way to use a condom, and there were significant differences by school type (16% in public schools and 44% in private schools). Linking information to sexual and reproductive health services outside of the classroom is an essential component of a comprehensive sexuality education program, but only 52% of teachers reported providing information about health services where adolescents could obtain contraceptive methods or counseling.
Class environment
Teachers face a multitude of challenges when teaching topics related to sexuality education. In key informant interviews, individuals reported that some teachers had reservations and inhibitions that made it difficult for them to teach sexuality-related topics. For instance, some teachers were embarrassed to mention reproductive organs by name, leading them to gloss over critical details. Key informants attributed this reticence in part to the fact that relationships between teachers and students were often akin to parent-child relationships, which could lead teachers to experience inhibitions similar to those that constrain parents in discussing sexuality with their children. Nonetheless, one key informant believed that teachers must meet their responsibility:
"Those who are embarrassed have got no place in teaching sexual education, they have to have it in them and be ready to impart knowledge whereby children are free to ask questions [and] interact. I think I stood once in a class and the teacher said [something] like, ‘This is a penis, trrarrara, I hope there are no questions.’"
—Respondent from a professional medical association
Results from the teacher survey also revealed challenges that teachers face in the classroom: Fifty-two percent had experienced lack of resources or teaching materials; 46% had struggled with lack of time; 38% reported lack of training or sufficient knowledge; 37% had experienced embarrassment about topics or terms; and 27% had to teach topics that they felt contradicted religious, traditional and personal beliefs or values (Table 4.12; Figure 4.13). Notably, 31% of teachers had experienced pushback or opposition from students, while 14% had experienced the same from parents or the community.
Findings from the student survey indicate that students’ perceptions of the class environment vary. While a majority of students perceived there was overall excitement to learn about sexuality education (72%), nearly half noted embarrassment to talk about the topics (Figure 4.14). Almost one-third of students overall cited overcrowding in their class as a challenge, more so in Homa Bay (45%) and Mombasa (38%) than in Nairobi (21%). Students’ perceptions of the authority their teachers hold or the competence with which they teach can play a role in their learning experience. One-fifth of students had the impression that their teacher was embarrassed to talk about topics related to sexuality education, and one-tenth perceived that their teacher did not know enough about the topics.
Adolescence is a transitional time during which many questions about the body, sexuality, relationships and a range of other topics related to SRH will be raised. Students need the freedom to express doubts and ask questions about these issues in order to absorb and connect with what they are learning. However, students may face challenges in the classroom: Half of surveyed students reported having experienced situations in which they wanted to ask a question in class related to sexuality but were too embarrassed. Thirty-two percent of students were afraid to offend or embarrass someone, and 23% were afraid that the teacher or other students would shut them down. One-fourth of all students reported that they never had a question that they did not ask. The proportions of students citing the various reasons for not asking questions in class differed significantly across counties; in general, students in Homa Bay were more likely than other students to cite a given reason.
Monitoring and evaluation
Because there is no stand-alone sexuality education course in Kenya, there is no clear standardized mechanism for monitoring or evaluating its teaching on a national level. Rather, any oversight of sexuality education topics is conducted under the monitoring or evaluation of the subject in which the topics are covered (e.g., biology). Key informant interviews revealed that multiple government institutions are mandated to monitor the implementation of government policies and curricula in schools. Those tasked with monitoring schools include the Ministry of Education (quality assurance department) and the Kenya Institute of Curriculum Development at the national level, and county education offices and head teachers at the county and school levels.
Key informants reported that community-based organizations actively engage schools to monitor how sexuality education is offered, and evaluate programs to the extent possible. Results from these small monitoring and evaluation initiatives are used in advocacy efforts (e.g., on issues of curriculum change), though it was observed that some civil society organizations are sanctioned by the Ministry of Education to report findings in schools and others are not, and therefore the government may not utilize their evaluation efforts equally across the country.
Our survey of schools assessed whether teachers were evaluated for their teaching of sexuality education at the individual school level (e.g., evaluated by school administration or principal), despite the lack of a national-level monitoring system. According to principals, about 57% of schools evaluate teachers on their teaching of sexuality topics in some capacity at least once a term (Table 4.13). However, teachers were never evaluated in 39% of schools. Those that did conduct evaluations used classroom observations (78%), written assessments (42%) and oral assessments (36%). Teachers reported being supervised by the school administration (49%) and school inspectors (27%) in their teaching of sexuality education, and half of teachers said they were monitored once during each term through class observation or oral or written assessment (not shown). Regarding student assessment, teachers reported that students were more commonly assessed on knowledge (in 95% of schools) than on practical skills (77%) or attitudes (74%), and that this testing was done through the subject exams in which the topics were integrated. Students were more commonly assessed on attitudes in public schools (91%) than in private schools (59%).
Summary of findings
- According to teachers, three-fourths of schools cover all topics that constitute a comprehensive curriculum, although teachers may be overreporting the topics taught. In contrast, only 2% of students reported learning about all of these topics in school.
- According to both teachers and students, virtually all schools cover concepts related to HIV and AIDS. Much less emphasis is placed on contraception and pregnancy prevention, particularly communication and practical skills related to contraceptive use.
- Messages conveyed by teachers are highly moralistic and focused on abstinence, emphasizing that sex is dangerous and immoral for young people as opposed to focusing on safer sex practices.
- About eight in 10 teachers reported teaching about contraceptives. Of these individuals, 98% taught about condoms and 61% about the pill, while fewer than half taught about other methods.
- Nine in 10 teachers reported teaching about abstinence, 71% of whom taught that it was the best or only method to prevent STIs and pregnancy.
- Only one-fifth of students reported learning about contraceptive methods, while two-thirds said they would like to learn more about them. One-tenth of teachers showed contraceptive methods to students so they could see how they work.
- Teachers and students reported challenges in the classroom that affect the teaching and learning of sexuality education. Both groups reported having experienced some embarrassment regarding sexuality education; and while most students were excited to learn about the topics, teachers said some common challenges were a lack of resources or materials; a lack of time, training or knowledge; and student opposition.
- The monitoring of sexuality education in schools suffers from inadequate attention and numerous barriers. Since topics are part of examinable subjects, coverage of the syllabus implies coverage of topics related to sexuality education. However, there are currently no tools to specifically monitor or evaluate the teaching of sexuality education in schools, or to assess students’ knowledge, attitudes and practical skills.
- Comprehensive sexuality education should include the fostering of practical skills; however, these receive little attention in the curriculum content and teaching approach, and student assessments focus more on knowledge than on attitudes and practical skills.
Chapter 5: School System Support for Sexuality Education
Improving the content of curricula, ensuring that teaching methods are adequate and conducive to learning, and establishing monitoring systems to ensure quality are essential to improving sexuality education in schools, but the quality of the teaching ultimately depends on the preparedness, confidence, knowledge and skills of teachers. Adequate training in the content, as well as in teaching methods and approach, of topics related to sexuality education is essential for teachers. An enabling and safe school environment has also been identified as a key component to a successful sexuality education program.39 This chapter presents quantitative and qualitative findings on these issues.
Teacher training
Secondary school teachers in Kenya are required to complete three years of teachers’ college at an accredited institution, and the latest revision of teachers’ education syllabi (2004) includes topics related to sexuality education, such as HIV and AIDS, drug and substance abuse, human rights and gender awareness.50
Since sexuality education is not a separate subject in schools, specialized pre-service training is limited. Key informants indicated that teachers’ knowledge of topics related to sexuality education is often inadequate, a sign that further training is needed. Some informants highlighted the additional need for teachers to be well-versed in the context regarding adolescent SRH in the country—for example, statistics on early sex, marriage and childbearing, and the prevalence of HIV and other STIs—to fully understand "the weight of the matter" when delivering this type of material. Several key informants shared the following observations:
"I have sat in a class where it looked like the teacher has no clue of what they are trying to teach.… We have to inform our teachers on how to do research, how to look for more information, [the same as when] the person who is standing to talk about geography knows everything about geography and not only a few things. And so when you are talking about … sexual and reproductive health, and rights,... you cannot say ‘Oh, I know nothing about the rights’—Go and research and come back and talk on the point with information."
—Respondent from a civil society organization
"When you are training, at first when you call them for the workshop they are like, ‘Ahh, we know these things, you know.’ They are like, ‘Aren’t these things about biology that we know?’ Because most of the time you find the biology or science teacher coming in, but by the end of the three days they tell you ‘There is so much that we didn’t know’ or they knew but didn’t know how to approach it."
—Respondent from a civil society organization
"They have not been given tips on how to handle the subjects so they end up being challenged; they will [present] the information, but the activities which they are supposed to work on with the learners will be a challenge for them.… You may find that there are [a] few teachers who are trained in that area or who are able to give that information [because they received] pre-service in college, [but] even the in-service has to be continued throughout for them to gain the confidence."
—Ministry of Education respondent
There are some challenges to training teachers on sexuality education: Funding for training is scarce and teachers may not be motivated or have time to dedicate to training while also covering their regular course load. Some teachers consider teaching these topics to be an extra burden. In situations where civil society organizations offer to train teachers, and even offer training stipends, the school heads may determine the content of the training and which teachers can attend. These teachers are in turn expected to train others, but because of time constraints, they may not be able to transfer the content of the training in its entirety. In some schools, only head teachers are funded to receive training, yet many are not directly involved in teaching SRH. Meanwhile, other teachers who are directly involved may have to pay out of pocket to attend, making training inaccessible to those who need it most. Moreover, according to key informants, teacher training offered by civil society organizations may follow an agenda that is specific to that organization, and may target only their key areas of interest. In addition, some trainings are limited to schools that are affiliated with the implementing organization, which can result in varying quality and content.
In the school survey, 85% of principals stated that teachers are required to receive pre-service training before teaching sexuality education topics, but only 8% of principals perceived that pre-service training was "very adequate" in preparing teachers (not shown). Seventy percent of teachers had received the relevant pre-service training (Figure 5.1), yet only 46% had received any related in-service training (Figure 5.2). Nine percent had received in-service training within the past year, 22% between one and three years ago, and 15% more than three years ago. Detailed findings on teacher training are presented in Table 5.1.
Three-fourths of teachers who had received either pre-service or in-service sexuality education training reported that the training covered at least one topic in each of the five thematic SRHR categories (a "minimum" level of comprehensiveness in the range of topics covered). Fifty-eight percent had received training on nearly all topics in each category (an "adequate" level), and 36% had received some training on all topics (a "high" level; Table 5.2).
Teaching support
Support and resources available to teachers
Most teachers had access to materials such as textbooks, teaching manuals, syllabi and clear objectives for teaching topics related to sexuality education, but fewer than half had access to plans or tools for how to evaluate or assess students on these topics (Table 5.3). The majority of teachers (73%) reported having support from other teachers. Nearly all principals (99%) said they supported teachers of sexuality education in some way, including by organizing meetings with them to discuss or resolve issues or concerns (70%); voicing support for sexuality education and for teachers at board meetings, parent-teacher association meetings and other community events (50%); and inviting outside experts to support teachers (59%).
However, teachers said they wanted additional assistance in various forms to help them teach more effectively; more than half desired more training and more teaching materials and strategies (Table 5.4; Figure 5.3). Some of the topics that teachers wanted more help with were positive living for youth with HIV, the prevention of violence and sexual abuse, female genital mutilation, and contraceptive methods and how to use them (Table 5.5; Figure 5.4).
Teachers’ perceptions of support
Support from authority figures and other stakeholders is important for effective sexuality education. The vast majority of teachers perceived that both the principal and other teachers were supportive in their teaching of sexuality education (89% and 96%, respectively—Figure 5.5; Figure 5.6). However, about a third felt that parents were unsupportive (Figure 5.7). A small proportion of teachers (17%) had experienced actual opposition or pressure from parents, community members, religious leaders or groups, government regulations or the school administration that they believed negatively affected their teaching of sexuality education (not shown).
School environment
A safe school environment is essential for fostering learning, and especially so for sensitive topics related to sexuality. Moreover, it is important to have an environment that is supportive toward reproductive and sexual rights. Almost all schools (98%) in the study have a child protection policy (Table 5.6). Policies are also in place regarding the treatment of students who either get pregnant or get someone pregnant, and to protect students from harassment by teachers and other students. The implementation of such policies contributes to the safety of the school environment and its conduciveness to sexuality education.
Clear policies and guidelines exist in Kenya to direct education-sector responses regarding pregnancies in schools. In accord with the Return to School Policy guidelines (1998), pregnant individuals are not allowed in schools, but are allowed to return to school (preferably a different school) after giving birth.51 According to principals in 52% of schools, an individual who becomes pregnant while attending school would be allowed to continue her studies. A large proportion of schools have some type of disruptive consequence (i.e., being asked to stay home or transfer to a different school) for students who become pregnant (48% of coeducational and females-only schools) or get someone pregnant (40% of coeducational and males-only schools). Consequences differed across counties, and private schools were stricter on males than were public schools. While most schools had strict guidelines for teachers and students who were found to be harassing students, some were more lenient (e.g., gave several warnings without expulsion or suspension).
Students’ perceptions of their own physical and emotional safety in school were mixed (Table 5.7). A third of students said they never felt safe expressing themselves in front of other students or teachers at their schools, and this sentiment was more common in Mombasa county than in Nairobi or Homa Bay county. More than half of students reported that they sometimes or always feared that other students or teachers may make fun of them or tease them at school, and a third reported sometimes or always feeling afraid that other students will physically harm them. Females were less likely than males to feel physically safe or safe expressing themselves in school.
One theme that emerged from the key informant interviews was the idea that teachers may contribute negatively to the emotional safety of students in the school. It was widely observed that some teachers lacked the professional competence to observe requisite norms, such as privacy, confidentiality and empathy, when handling sexuality matters or student concerns. One civil society respondent described how one teacher had breached confidentiality by asking a student, in front of the whole class, about a sensitive issue for which guidance had been sought:
"[The] teacher came to class and said, ‘Elizabeth, can you tell us about rape, you, you were even raped, can you tell us about the rape issue so that you can give an example so that these girls can stop roaming aimlessly.’"
—Respondent from a community-based organization
Summary of findings
- Some teachers lack the training to teach sexuality education topics. Although 85% of schools required teachers to have pre-service training, only 70% of teachers had received it. A mere 8% of principals perceived that this training was very adequate, and 68% of teachers felt they needed more training.
- Fewer than half of teachers had received any in-service training. These programs sometimes offer opportunities to increase teachers’ skills and enthusiasm to teach sexuality education, but resource constraints have limited the number of teachers that can be trained. This type of training is not standardized across the country, and is often provided by civil society organizations that have specific agendas and narrow catchment areas.
- The majority of teachers had access to resources such as curricula and teaching manuals to support their teaching, and for many, media sources such as the Internet were an important resource. However, many teachers desired more materials, information and training (particularly regarding violence prevention and contraceptive methods) to enable them to teach more effectively.
- While teachers overwhelmingly said that principals were supportive of sexuality education, a third of teachers perceived parents to be unsupportive, and nearly one in five had experienced opposition from the community.
- School policies offer a supportive environment for adolescents to learn about sexuality education; most schools have child protection and anti-harassment policies, although these are far from standardized or uniformly implemented. Despite these policies, a third to a half of students did not feel safe expressing themselves in front of others at school or feared being teased or even physically harmed. Such pressures and concerns may impede a student’s curiosity and ability to learn about sexuality and SRH.
Chapter 6: Out-of-school Sources for Sexuality Education
Evidence suggests that while school may be an ideal setting for sexuality education, many adolescents receive additional information about these topics outside of the classroom. Understanding what sources are most used and most trusted by adolescents has important programmatic implications. This chapter presents qualitative and quantitative findings on alternative sources of SRH information used by young people and on out-of-school activities related to sexuality education.
Alternative sources
Students navigate a constellation of competing and sometimes conflicting sources of SRH information outside of school, ranging from family members to media sources. A notable 94% of students reported receiving information on sexuality education topics from media sources, including books, pamphlets, the Internet, radio and TV; 86% from friends, girlfriends or boyfriends; 72% from their mothers; 70% from health centers, youth centers or other community centers; and 39% from their fathers (Table 6.1). There were significant differences by gender: Females were more likely to receive information from their mothers, other family members and after-school programs, and males were more likely to receive information from their fathers. The top source of SRH information most commonly cited by males was the media, followed closely by fathers and mothers (Figure 6.1). The top source for females was their mothers.
Among students who had participated in out-of-school activities, the most frequently cited were seminars and talks (71%), peer education groups (59%) and debates (38%; Figure 6.2). About a quarter of students said they participated in nonschool activities at least once a week, and another quarter engaged in such activities at least once a month; four in 10 did so every few months or once or twice a year (Figure 6.3).
Key informants reported that various media channels are used in Kenya to educate adolescents and young people about SRH issues within their communities. In particular, media programs educate youth about their reproductive health, rights and choices (e.g., regarding pregnancy, abortion and STIs, as well as the correct use of contraceptive methods). Furthermore, the media are able to identify experts in reproductive health to provide informed views, and can also shape the reproductive health agenda for adolescents through advocacy, mobilization of resources and facilitation of dialogue among stakeholders from the community level to the national level.
However, some key informants shared negative perceptions about the media’s role in influencing adolescents’ attitudes and behaviors. One informant described the following concerns: "I think the media are in business … and sex pays. Sex sells. If you listen to the morning radio, even [in] daytime it is all about sex, talking about Facebook, social media. We have nudity all over the place. As a parent, it is very difficult to monitor what your kid is doing, but the most important thing, for me I think, [is that the] media should be more responsible.… As adults we should give our children knowledge to choose the kind of media to attend to."
—Respondent from a community-based organization
NGOs and community-based organizations
NGOs, professional medical organizations and community-based organizations (CBOs), as well as women’s, men’s and youth groups, also play a critical role in teaching adolescents about health and sexuality. A CBO respondent emphasized that youth groups have brought information to the community on specific topic areas—such as sexual and gender-based violence and HIV prevention—through cooperative activities like sports tournaments or other community engagements in which all members of the community, including parents, are invited to participate. However, while CBOs can potentially improve access to information and contribute to sensitization efforts, the quality and comprehensiveness of the information are not regulated and may vary by organization. For example, some of these CBOs insist on abstinence, or withhold comprehensive information about sexuality:
"And so when we teach them about their reproductive organs, when we tell them ‘You are a girl and you have a vagina,’ at that age when you are still underage, [we tell them] that your vagina is meant for urination, so she comes up knowing that the work of the vagina is only for urinating."
—Respondent from a women’s group
NGOs also support advocacy on school readmission policy for teenagers who got pregnant (or got someone pregnant), and for the training of teachers on SRH issues. Certain religious institutions were involved in disseminating information on SRH, for example, through youth classes. However, some of these institutions reportedly influenced their members not to use condoms or contraceptives and emphasized abstinence.
Summary of findings
- Although there are many sources of SRH information available to adolescents, the quality of the information they receive outside of school is unknown, and some sources may perpetuate negative attitudes or misinformation about key topics.
- The media—including the Internet—were a key source of out-of-school information on SRH topics; almost all students said they had used media. Indeed, the Internet was the most commonly used source of information for males, followed closely by fathers and mothers. By far the top-rated source for females was their mothers.
- Respondents from civil society organizations cited the media as key to disseminating SRH information to both youth and the wider community and to offering young people a platform with which to voice their opinions and ideas about sexuality. Yet some also blamed media channels for exposing adolescents to sex-related content they deemed inappropriate.
- Much of the community-level advocacy and public education regarding SRH is provided by community-based organizations, including women’s and youth groups. However, it is important to note that some of their messages may withhold key information about sexuality in favor of an abstinence-only agenda.
Chapter 7: Opinions About Sexuality Education
To gain a holistic understanding of the context in which sexuality education is taught in Kenya, and of the support or opposition that such programs face, it is important to explore the opinions of both students and teachers regarding sexuality education, as well as the perspectives of the wider community.
Students’ opinions
Almost all students (99%) believed that sexuality education should be taught in schools (Table 7.1). However, students were not asked what type of sexuality education should be taught, for example, whether it should emphasize abstinence or be comprehensive. The main reason for their support was the need to know how to avoid getting HIV or other STIs (cited by 69%). Considerable proportions cited other reasons, and there was variation among the three counties. The higher proportions of students citing many of the reasons in Homa Bay county than in Nairobi and Mombasa counties likely reflect the relatively high risks of unintended pregnancy and HIV in that region, which perhaps lead students to recognize the multiple benefits of sexuality education in addressing various issues that they perceive as prevalent in their area (Figure 7.1).
In general, students’ opinions regarding the sexuality education they received were positive: The vast majority (93%) reported that it had been useful or very useful in their personal lives. Seventy-one percent of students said they enjoyed classes on sexuality education more than those on other subjects, while 25% enjoyed them about the same.
Principals’ and teachers’ opinions
Nearly all principals and teachers supported sexuality education, although they were not asked to distinguish between the types or the moral stances of programs (e.g., whether focused on abstinence or comprehensive), or to specify the range of topics that should be included. On the basis of teachers’ responses regarding content in Chapter 4, it is likely that some favored a strict abstinence-based approach, which is not support for a comprehensive program. A subsequent question about specific topics brought some nuance to the picture. While most teachers were in support of most topics being taught, some opposed teaching certain critical issues that would be expected in a comprehensive program. For example, 31% did not support teaching where to get contraceptives, 28% did not support teaching how to use contraceptives and 22% opposed teaching the negative implications of engaging in sex in exchange for money or gifts (not shown).
When asked about the main messages that sexuality education should impart, 66% of teachers agreed with the statement that "abstinence is the best way to prevent pregnancy and STIs/HIV," and 63% agreed that "everyone deserves respect, no matter what gender, race or social status." This latter sentiment was particularly common in Mombasa, where 86% of teachers felt that this was an important message, compared with 60% in Nairobi and 50% in Homa Bay. Almost half of teachers thought one of the most important things to impart was information about STI and HIV transmission and where to access services; only 21% placed high importance on accurate information about contraceptive methods and where to access them. Eighty-six percent of teachers believed that sexuality education seeks to impact students’ knowledge, while 61% identified attitudes; smaller proportions identified practical skills, self-confidence or opinions (Figure 7.2).
The attitudes held by teachers and principals may influence the teaching of sexuality education, and in turn impact students’ learning experience and ultimately shape their attitudes, knowledge, behavior and sense of agency. Large majorities of principals (83%) and teachers (77%) believed it was important to tell students where to access SRH services (Table 7.2). More than half of principals (54%) and teachers (66%) believed in the importance of teaching students about contraceptive methods. However, both groups also held highly conservative attitudes regarding sexuality among adolescents. Almost all agreed that males and females should remain virgins until marriage (92‒93%), and that sexual relationships should only be between a man and a woman (95‒96%). Substantial proportions of principals (45%) and teachers (36%) agreed that youth who carry condoms are bad, promiscuous or unfaithful. In addition, 38% of principals and 24% of teachers believed that using a condom is a sign of not trusting your partner, and most principals and teachers held the misconception that making contraceptives available encourages young people to have sex (62‒74%).
Perspectives of government, civil society and community members
Most respondents observed that adolescents were at elevated risk for negative SRH outcomes, and supported some form of sexuality education. Key stakeholders noted poor parent-child communication regarding sexuality; high rates of unsafe abortion, HIV and STIs among young people; increased access to prohibited sexually explicit materials; high incidence of sexual violence; and the existence of several myths and mistaken beliefs related to sexuality. Appropriate and focused implementation of existing sexuality education policies and guidelines was considered essential to improving knowledge and health outcomes among young people. A county official commented on young people’s interest in learning about their sexuality:
"If you are a keen teacher you’ll realize that learners are quite attentive when you start mentioning these things to them. They get interested because they want to know more, it’s like they don’t have information about themselves, and especially, when they reach certain stages, maybe adolescence, they want to know why, why are these changes coming up?… They would even request some teachers to repeat the topic."
—Respondent from a county education office
Government respondents emphasized that sexuality education would help prevent unintended pregnancies, improve school participation and performance, reduce rates of HIV infection, deter gender-based violence and support healthier growth and development among young people. Sexuality education was also viewed as critical to delaying the onset of first sex, reducing unsafe abortion, decreasing unintended childbearing and ensuring a successful transition to adulthood. One government official drove this point home:
"If you look at the indicators in Kenya today, they are not amusing at all, and we believe that if young people are able to access that information in schools even before they get to puberty, even before they become sexually active, then they are able to make informed choices."
—Government official
While most key informants believed that sexuality education was important, there were differing opinions on who should be responsible for teaching adolescents about these issues. Respondents suggested that although parents may expect that their children will learn sexuality education in school, at least supplementally if not primarily, some teachers expect parents to provide this information at home, leading to an information gap among adolescents. Most respondents across the community, civil society and government agencies preferred that parents be the first to provide sexuality information to their children, because of their pivotal role in early childhood development. However, some observed that "this is a conversation that is not happening." Indeed, while student respondents felt that their parents supported sexuality education, a member of a youth organization opined that discussing topics related to sexuality was difficult for parents, who often feel embarrassed or do not want to admit that their children need such information.
Yet even among those who preferred that parents play the role of primary educators on these topics, many believed that parental responsibility should be augmented by other sources in school, community and even religious institutions:
"In my opinion, the information should not start in schools, it should start at home. Parents should talk to their children, tell them [that sexuality] is a private area, tell them no one should breach any area of your privacy.... So in school this can be reinforced when the child is five, six [or] seven years of age."
—Respondent from a professional medical association
Other respondents preferred that teachers provide sexuality education first and foremost, and cited parents’ lack of skills to deliver sexuality information appropriately. School-based sexuality education was considered a solution to the unreliable information available to young people through other sources, and as essential to helping young people develop capacity, self-efficacy, responsibility and resilience. Such education was also considered important in efforts to improve youth appreciation that sexuality is a normal component of their everyday lives, as they discover and experience themselves as gendered and sexual people at this pivotal stage.
The relationship between teachers and students was recognized as a unique entry point for school-based sexuality education. In an environment in which communication about SRH issues between parents and children is virtually nonexistent, teachers fulfill a key role. In schools, students look up to teachers as authorities, view them as knowledgeable and well-informed, and turn to them for accurate information on a range of issues—all of which highlight the imperative that teachers be adequately trained to provide this information.
Some community-level respondents preferred that the local community provide sexuality education, because of its cultural role in shaping behaviors and norms. Examples were given of how elders in the community would guide youth regarding societal norms and expectations of gendered roles. However, it was noted that these relationships were collapsing and that society was tending toward a more "individualistic" orientation. Community health workers§§§ were preferred by some as purveyors of sexuality education because they can act as resource persons to link adolescents to support services. Other community institutions, such as churches, were also considered important owing to the influence that religious teachers have over their congregations and the opportunities to organize youth for educational sessions. However, some respondents observed that religious groups could also undermine sexuality education, for example, through prohibition of discussions about sexuality, insistence on virginity and abstinence, and teaching against contraceptives.
Summary of findings
- Nearly all principals, teachers and students supported sexuality education being taught in schools.
- Students had favorable views about the sexuality education they had received in schools: Almost all considered it useful or very useful in their personal lives. Nearly a third of students reported that they did not receive this information from their parents.
- Most teachers believed that sexuality education should impact students’ knowledge and attitudes. Fewer believed that it should impact practical skills or self-confidence.
- While many teachers placed high importance on teaching about the prevention of HIV and STI transmission, few perceived the importance of providing accurate information about contraceptives and where to access them.
- Teachers held negative attitudes and misconceptions about a range of issues related to adolescent sexuality; these may negatively influence the content and manner of teaching specific topics.
- Key informants expressed their support for sexuality education, but emphasized the need for better teacher training to equip individuals with the knowledge and capacity to address key sensitive issues with professionalism and empathy.
- Key informants expressed conflicting views regarding who should be teaching sexuality education to adolescents. Some believed teachers were the most appropriate, pointing to the authority and trust that adolescents place in them. Others thought parents should be the primary source of information, but conceded that the latter might lack the tools to effectively and accurately talk to their children about these issues.
- Certain respondents advocated for the role of community members, such as grandparents and community health workers, as well as the church, as traditional sources of information with deep knowledge of societal norms and expectations. However, some respondents cautioned that religious dogma (i.e., prohibition of discussion of sex and insistence on virginity and abstinence) may undermine comprehensive sexuality education.
Chapter 8: Conclusions and Recommendations
Adolescent sexual and reproductive behavior is a highly debated topic in Kenya, and rights-based initiatives are often challenged by traditional and conservative abstinence-promoting perspectives. Findings from this study demonstrate the Kenyan government’s commitment to provide sexuality education, as reflected in the development and revisions of policies and curricula related to adolescent sexual and reproductive health. Yet challenges remain—from the national policy-making and program-planning level down to the classroom implementation level.
The comprehensiveness of policies and curricula has continuously fallen short because of challenges posed by highly conservative societal norms and cultural sensitivities regarding the inclusion of topics such as contraception, abortion and sexual orientation. In the classroom, poorly trained teachers continue to struggle with teaching sensitive topics. The lack of comprehensiveness in topic coverage, the fear-based orientation in the teaching and the consistent negative light cast on adolescent sexuality are barriers to a successful sexuality education program. While there is potential for providing an effective learning experience, clear steps should be taken to demystify and desensationalize sexuality among adolescents, and both the development of comprehensive policies and programs and their implementation need to be improved for the full benefits of this education to be reaped by adolescents. Evidence continues to show that adolescents in Kenya lack adequate knowledge and skills to help them live healthy sexual and reproductive lives.
Lessons from the classroom
Support for sexuality education in schools
There is a widespread perception that the community and parents are opposed to sexuality education. However, our study showed that there is strong support for sexuality education on the part of students, teachers, principals and members of the community, and a persistent desire and enthusiasm among students to broaden their knowledge on a range of sexuality education topics. Students in particular had favorable views about school-based sexuality education: Almost all considered it useful or very useful in their personal lives. Overall, parental opposition was very low, and key informants did not perceive community opposition to be a major challenge; rather, lack of funding and teacher training, and opposition by specific influential religious groups, were identified as key obstacles. While some community members claimed that the responsibility of providing sexuality education should fall on parents, many students reported that they do not receive this information at home.
Lack of comprehensiveness of the curriculum
Despite reports by teachers that a majority of schools teach all topics that make up a comprehensive program according to international standards, a negligible proportion of students reported learning about all of the core sexuality education topics in school. The most current evidence suggests that participatory sexuality education programs that include content on gender equality, power relations and human rights are more likely to be associated with positive SRH outcomes than are programs that do not.12 According to both teachers and students, virtually all schools teach about HIV and AIDS, but less emphasis is placed on essential topics regarding contraception and pregnancy prevention (particularly communication and practical skills related to contraceptive use), as well as on gender relations, equity and rights. Yet "communication and negotiation," practical skills, and gender and rights issues feature prominently in the UNFPA definition of comprehensive sexuality education used in this study (see Chapter 2). The definition also emphasizes that CSE should "equip children and young people with the knowledge, skills, attitudes and values that will enable them to develop a positive view of their sexuality." However, the current practice in Kenya largely ignores skills-based learning, and the attitudes and values nurtured by the program do not facilitate a positive view of sexuality; indeed, the messages conveyed by teachers are often highly conservative and focused on abstinence, emphasizing that sex is dangerous and immoral as opposed to focusing on safer sex practices.
The evidence shows that abstinence-only programs are not effective in improving sexual and reproductive outcomes in adolescents.8,9 Virtually all teachers cover abstinence in their classes, and most emphasize that it is the best or only method to prevent STIs and pregnancy. In contrast, a minority of teachers highlighted the importance of conveying accurate information about contraceptives and where to access them. Few students reported learning about how to obtain or use contraceptive methods, but a majority expressed a desire to learn more about these topics, along with related communication skills. This suggests that the emphasis on abstinence at the expense of teaching more holistically about issues of sexuality is not only detrimental to students’ SRH in the long run, but also conflicts with students’ own assessments of what they need to know to safely navigate adolescence.
Inadequate teacher preparedness
Having competent educators—who approach adolescents with respect and encourage development of communication, negotiation and decision-making skills while delivering fact-based information—is crucial for effective programs. The training of a large number of teachers requires significant ongoing investment, and this is a challenge in Kenya. Individuals who implement sexuality education, as well as other key stakeholders, have cited lack of teacher skill as the main obstacle to success and have identified investing in teachers’ capacities (through pre-service and in-service training) as a main priority.39 In Kenya, the educational system is already constrained, teachers are overstretched, and funding for training and materials is limited.
Often, only principals and a few teachers are funded to attend trainings on teaching sexuality education, with the expectation that they will then train others. However, in practice this rarely happens. While a sizable proportion of teachers reported receiving pre-service training, this is usually general and does not often include dedicated sexuality education modules, since sexuality education is not a stand-alone subject. Fewer than half of teachers received any ongoing in-service training, and a majority expressed the need for more training to adequately prepare them to teach sexuality education. Even among teachers who received training, they were rarely trained in all topics that are included in comprehensive sexuality education according to international standards. If these topics formed part of the compulsory curriculum and were examinable, this would necessitate their inclusion as a separate module in pre-service teacher training and might encourage more investment in in-service training on sexuality education.
Many teachers reported facing challenges in their teaching, including lack of resources or materials, lack of time, lack of knowledge or training, embarrassment and opposition from students. The last point is interesting in light of students’ overwhelming support for the subject, and may warrant further research to understand this discrepancy. Furthermore, the successful implementation of sexuality education requires the use of more participatory pedagogic methods than those to which schools or teachers may be accustomed. As seen in the school survey, very few teachers reported using interactive methods such as condom demonstrations (most used lectures and talks), and very few placed a strong emphasis on developing practical skills or self-confidence. These shortcomings are borne out in students’ desires to learn more skills-based topics and use participatory teaching methods.
Teachers’ attitudes toward sexuality education
Many teachers reported negative attitudes and poor skills regarding SRH issues, indicating that further sensitization is needed. For example, more than half agreed that making contraceptives available encourages young people to have sex; more than one-third agreed that young people who carry condoms are bad, promiscuous or unfaithful; and about one-fourth agreed that using condoms is a sign of not trusting your partner. Despite these negative views, there is no evidence to show that talking about sex or informing adolescents about safer sexual practices prompts them to engage in sex.2,5 To the contrary, providing sexuality education in a timely manner, before adolescents are sexually active, can help prepare them to protect themselves from negative SRH outcomes when they do become sexually active. Experts now recommend that age-appropriate sexuality education be started earlier, well prior to sexual initiation,5 but too often this education arrives too late. Nationally, among adolescents, 11% of females and 20% of males have had sex before the age of 15,20 and as shown in this study, many adolescents in secondary school are already sexually active, as 15% and 42%, respectively, had already had sex at the time of the survey.
Perceived safety of the school and class environment
The success of a sexuality education program also depends on it being implemented in a safe environment where adolescents can freely express themselves without fear of harassment or reprisal. The study confirmed the existence of school policies aimed at promoting a safe and supportive environment for adolescents to learn about sexuality education; most schools have child protection and anti-harassment policies, although these are far from standardized or uniformly implemented. A glimpse into the classroom realities as experienced by teachers and students revealed the absence of an emotionally safe space for students to explore sensitive topics, and this poses another challenge to the effectiveness of sexuality education in schools and dampens the benefits that CSE is currently offering adolescents in Kenya. Despite these protective policies, nearly half of students did not feel safe expressing themselves in front of others at school, and feared being teased or even physically harmed in their classes on sexuality education. Teachers may contribute to the negative classroom environment by addressing students inappropriately or exposing confidential information. This may impede a student’s curiosity, confidence and ability to learn about sexuality and reproductive health in general.
The way forward
It is clear from the study findings that the Kenyan government has been open to educational reforms, and policies do exist to support the provision of school-based sexuality education, but the government has not been successful in ensuring the implementation of these policies. Because sexuality education is guided by policies at multiple levels—from national laws to local school administrative guidelines—political and social leadership is needed at each level to support implementation. Appropriate coordination and synergy are also needed among the different government agencies involved to ensure uniformity and better utilization of the available resources.
While NGOs have developed more comprehensive sexuality education curricula, these are mainly used in extracurricular activities in schools in a few districts, may vary in quality and are not implemented uniformly in each school, leading to a disjointed program overall. Moreover, there is often minimal teacher training for implementing them, and teachers who are unprepared and lack knowledge or adequate support may limit their teaching to topics with which they are comfortable.
The sexuality education topics that are integrated into compulsory subjects are limited in scope, and life skills—the subject into which the widest range of topics are included—is not examinable. The fact that key sexuality education topics are not well integrated into compulsory and examinable subjects limits the information available to students and may also reduce the incentive for students and teachers to accord them high priority. In sum, high-quality comprehensive sexuality education needs to be recognized as essential for the healthy development of adolescents and their transition to adulthood, and needs to become institutionalized within national systems of education if it is to be delivered at scale on a sustained basis.
Developing, implementing and scaling up programs may require bureaucratic changes and coordination among government sectors and ministries, including those focused on education, health and youth. More coordinated efforts among ministries, county governments and civil society organizations, as well as with adolescents, are warranted in order to:
- Prioritize at the primary school level a comprehensive and rights-based focus for sexuality education to bring it in line with the commitment made in the 2013 ministerial declaration, thus ensuring that students receive essential age-appropriate information and develop skills prior to initiating sexual activity.
- Ensure that the development of policies, guidelines and curricula is based on the growing body of evidence documenting the characteristics of successful comprehensive sexuality education programs and the positive impact that they can have on adolescents when designed and delivered appropriately.
- Integrate a wider range of sexuality education topics into life skills, which should be included in the curriculum as an examinable subject, and ensure that sufficient time is allocated for teachers to cover those topics.
- Improve the comprehensiveness of the curriculum content and diversify the teaching methods used in the classroom to more accurately follow UNFPA’s definition of comprehensive sexuality education, and to place more emphasis on promoting practical skills, confidence and agency among students; eliminate fear-based and moralistic messages; and increase the focus on strategies for preventing unintended pregnancies that teach about a broad range of contraceptives (including long-acting methods) and negotiating skills within relationships.
- Improve teacher training—both pre-service and in-service—to ensure that teachers are up to date on the latest information, skills and techniques and have the support and resources necessary to confidently, accurately and effectively teach the sensitive topics related to sexuality education.
- Develop a mechanism for monitoring and evaluating the teaching of sexuality education in schools, and for assessing the gaps between policies and classroom realities on a yearly basis.
- Ensure coordination between programs run by the government, NGOs and other bodies, so that the lessons learned from effective NGO programs can be applied to the design and implementation of the government program at a national level.
FOOTNOTES
*Comprehensive knowledge includes correctly identifying that HIV risk can be reduced by consistently using condoms and by having a single partner who is HIV-negative and who has no other partners, knowing that a healthy-looking person can have HIV and rejecting the two most common local misconceptions about HIV transmission (via mosquitoes and sharing food).
†A large-scale study of the implementation of sexuality education curricula in schools in eight Asian countries has been undertaken by UNESCO, with technical support from the Population Council. No such multicountry studies are under way in Africa or Latin America.
‡The individual topics included in the categories are based on international guidelines, but the levels of comprehensiveness were defined specifically for this study and do not refer to any international standards.
§The education system in Kenya includes eight years of primary education (Standards 1‒8), four years of secondary education (Forms 1‒4) and four years of tertiary education. Secondary school students are, on average, between 13 and 17 years old.
**The list included data on all secondary schools, with specific information on location, type (public or private), ownership, coeducational status (mixed, females only or males only), enrollment and other key indicators.
††School stratification was based on the size of each stratum as generated using the same criteria. A random replacement sample was drawn, equally stratified by these criteria, to mitigate the possibility of any changes in school status since 2014.
‡‡Students’ questionnaires were self-administered in one room on the school premises under the guidance of three field interviewers.
§§This institute was established in 2013 as the successor to the Kenya Institute of Education. Details on the curriculum development process are provided at http://www.kicd.ac.ke/images/corpcomm/currdevcycle.pdf.
***The Kenya portion of the review assessed the 2008 Life Skills Education Syllabus Series, including the syllabi and teachers’ handbook for Primary and Secondary Life Skills Education; the syllabi and facilitators’ handbook for the 1999 Let Us Talk About AIDS series, which targeted children in and out of school; and the 2002 Lower and Upper Primary Life Skills Education Curriculum (Kenya Institute of Education).
†††The number of hours dedicated to sexuality education was estimated using teachers’ reports of the amount of time dedicated specifically to teaching any topics related to sexuality education (as defined in the study). While this estimate provides an idea of the overall number of hours, we do not know which particular topics are given more time or attention.
‡‡‡Measures based on teachers’ responses may be biased in either direction because of overreporting or underreporting, or because of reliance on one teacher’s response at a school regarding a noncompulsory course.
§§§Community health workers are local volunteers engaged at the lowest level of the health system. They provide reproductive health information to households, including information on contraception; they also help in the community distribution of condoms and pills.
REFERENCES
1. Biddlecom AE et al., Protecting the Next Generation in Sub-Saharan Africa: Learning from Adolescents to Prevent HIV and Unintended Pregnancy, New York: Guttmacher Institute, 2007, https://www.guttmacher.org/report/protecting-next-generation-sub-sahara….
2. Kirby D, Emerging Answers 2007: Research Findings on Programs to Reduce Teen Pregnancy and Sexually Transmitted Diseases, Washington, DC: National Campaign to Prevent Teen and Unplanned Pregnancy, 2007, https://thenationalcampaign.org/resource/emerging-answers-2007—full-report.
3. United Nations Educational, Scientific and Cultural Organization (UNESCO), Emerging Evidence, Lessons and Practice in Comprehensive Sexuality Education: A Global Review, Paris: UNESCO, 2015.
4. National Guidelines Task Force, Guidelines for Comprehensive Sexuality Education: Kindergarten Through 12th Grade, third ed., Washington, DC: Sexuality Information and Education Council of the United States, 2004, http://www.familiesaretalking.org/_data/global/images/guidelines.pdf.
5. UNESCO, International Technical Guidance on Sexuality Education: An Evidence-Informed Approach for Schools, Teachers and Health Educators, Paris: UNESCO, 2009.
6. United Nations Population Fund (UNFPA), Comprehensive Sexuality Education: Advancing Human Rights, Gender Equality and Improved Sexual and Reproductive Health—A Report on an International Consultation to Review Current Evidence and Experience, New York: UNFPA, 2010.
7. World Health Organization (WHO) Europe and Federal Centre for Health Education (BZgA), Standards for Sexuality in Europe. A Framework for Policy Makers, Educational and Health Authorities and Specialists, Cologne, Germany: WHO Europe and Federal Centre for Health Education (BZgA), 2010.
8. Kirby DB, The impact of abstinence and comprehensive sex and STD/HIV education programs on adolescent sexual behavior, Sexuality Research & Social Policy, 2008, 5(3):18–27.
9. Underhill K, Montgomery P and Operario D, Sexual abstinence only programmes to prevent HIV infection in high income countries: systematic review, BMJ, 2007, 335(7613):248, doi:https://doi.org/10.1136/bmj.39245.446586.BE.
10. Fonner VA et al., School based sex education and HIV prevention in low- and middle-income countries: a systematic review and meta-analysis, PLoS One, 2014, 9(3):e89692, http://dx.doi.org/10.1371/journal.pone.0089692.
11. Gallant M and Maticka-Tyndale E, School-based HIV prevention programmes for African youth, Social Science & Medicine, 2004, 58(7):1337–1351.
12. Haberland N and Rogow D, Sexuality education: emerging trends in evidence and practice, Journal of Adolescent Health, 2015, 56(1, Suppl.):S15–S21.
13. Haberland NA, The case for addressing gender and power in sexuality and HIV education: a comprehensive review of evaluation studies, International Perspectives on Sexual and Reproductive Health, 2015, 41(1):31–42, doi:10.1363/4103115.
14. Kirby D and Coyle K, School-based programs to reduce sexual risk-taking behavior, Children and Youth Services Review, 1997, 19(5–6):415–436.
15. Kirby D, Obasi A and Laris BA, The effectiveness of sex education and HIV education interventions in schools in developing countries, World Health Organization Technical Report Series, 2006, 938:103–150.
16. Béguy D et al., Status Report on the Sexual and Reproductive Health of Adolescents Living in Urban Slums in Kenya, STEP UP Technical Working Paper, Nairobi, Kenya: African Population and Health Research Center, 2013.
17. Ministry of Health and Ministry of Planning and National Development, Adolescent Reproductive Health and Development Policy Plan of Action 2005–2015, Nairobi, Kenya: Ministry of Health, 2005.
18. Obare F and Birungi H, Policy scripts and students’ realities regarding sexuality education in secondary schools in Kenya, Sex Education, 2013, 13(6):615–629.
19. African Population and Health Research Center et al., Incidence and Complications of Unsafe Abortion in Kenya: Key Findings of a National Study, Nairobi, Kenya: African Population and Health Research Center, 2013.
20. Kenya Bureau of Statistics et al., Kenya Demographic and Health Survey, 2014, Calverton, MD, USA: Kenya National Bureau of Statistics and ICF Macro, 2015.
21. Mumah J et al., Unintended Pregnancies in Kenya: A Country Profile, STEP UP Research Report, Nairobi, Kenya: African Population and Health Research Center, 2014.
22. National AIDS Control Council, Kenya AIDS Response Progress Report: Progress Towards Zero, Nairobi, Kenya: National AIDS Control Council, 2014.
23. Joint United Nations Programme on HIV/AIDS (UNAIDS), Global Report: UNAIDS Report on the Global AIDS Epidemic 2013, Geneva: UNAIDS, 2013.
24. UNAIDS, HIV prevalence, 2015, http://aidsinfo.unaids.org/.
25. Kenya Law Reports, Prohibition of Female Genital Mutilation Act No. 32 of 2011, Nairobi, Kenya: National Council for Law Reporting with the Authority of the Attorney-General, 2011.
26. UNESCO, Levers of Success: Case Studies of National Sexuality Education Programmes, Paris: UNESCO, 2010.
27. UNESCO, Regional Diagnostic Report on Education and Services for Sexual and Reproductive Health of Adolescents and Young People in Eastern and Southern Africa, Paris: UNESCO, 2013.
28. Ministerial Commitment on comprehensive sexuality education and sexual and reproductive health services for adolescents and young people in Eastern and Southern Africa, 2013, http://hivhealthclearinghouse.unesco.org/sites/default/files/resources/….
29. Plan USA, Sexuality Education in Asia: Are We Delivering? An Assessment from a Rights-Based Perspective, Bangkok, Thailand: Plan USA, 2010.
30. Hunt F and Monterrosas Castrejón E, Evaluación de la Implementación de la Declaración Ministerial Prevenir con Educación: Del Acuerdo a la Acción. Avances el Latinoamérica y el Caribe, 2012, https://www.coalicionmesoamericana.org/node/3.
31. UNESCO and UNFPA, Sexuality Education: A Ten-Country Review of School Curricula in East and Southern Africa, New York: UNESCO and UNFPA, 2012.
32. UNESCO Bangkok, Review of Policies and Strategies to Implement and Scale Up Sexuality Education in Asia and the Pacific, Bangkok, Thailand: UNESCO Bangkok, 2012.
33. United States Agency for International Development (USAID), Making Comprehensive Sexuality Education Available at a National Scale: A Case Study About Tailoring International Guidance for Kenya, Washington, DC: USAID, 2012.
34. Agbemenu K and Schlenk EA, An integrative review of comprehensive sex education for adolescent girls in Kenya, Journal of Nursing Scholarship, 2011, 43(1):54–63.
35. Njue C et al., "If you don’t abstain, you will die of AIDS": AIDS education in Kenyan public schools, AIDS Education and Prevention, 2009, 21(2):169–179.
36. UNESCO, Young People Today: Time to Act Now, Paris: UNESCO, 2013.
37. UNESCO and UNAIDS, 2011–2012 Education Sector HIV and AIDS Global Progress Survey: Progression, Regression or Stagnation? Paris: UNESCO, 2013.
38. International Planned Parenthood Federation, Inside & Out: A Comprehensive Sexuality Education Assessment Tool, 2013, http://www.ippf.org/resource/Inside-Out-Comprehensive-Sexuality-Educati….
39. UNFPA, Operational Guidance for Comprehensive Sexuality Education: A Focus on Human Rights and Gender, 2014, http://www.unfpa.org/publications/unfpa-operational-guidance-comprehens….
40. UNFPA Expert Group, The Evaluation of Comprehensive Sexuality Education Programmes: A Focus on the Gender and Empowerment Outcomes, 2015, http://www.unfpa.org/publications/evaluation-comprehensive-sexuality-ed….
41. UNESCO, International Technical Guidance on Sexuality Education: An Evidence-Informed Approach for Schools, Teachers and Health Educators, Paris: UNESCO, 2009.
42. Landry DJ, Kaeser L and Richards CL, Abstinence promotion and the provision of information about contraception in public school district sexuality education policies, Family Planning Perspectives, 1999, 31(6):280–286.
43. Landry DJ, Singh S and Darroch JE, Sexuality education in fifth and sixth grades in U.S. public schools, 1999, Family Planning Perspectives, 2000, 32(5):212–219.
44. Centers for Disease Control and Prevention (CDC) and WHO, Global School-Based Student Health Survey (GSHS), 2009, http://www.cdc.gov/GSHS.
45. Profamilia, Encuesta Nacional De Demografía y Salud 2010, Bogotá, Colombia: Profamilia, 2011.
46. CDC, School Health Policies and Practices Study, 2015, http://www.cdc.gov/healthyyouth/data/shpps/questionnaires.htm.
47. Kenya Institute of Education, Life Skills Education Syllabus, Nairobi: Kenya Institute of Education, 2002.
48. Kenya Institute of Education, Secondary Education Curriculum: Life Skills Education Syllabus, Nairobi: Kenya Institute of Education, 2008.
49. Network for Adolescents and Youth in Africa (NAYA), Assessment on the Effectiveness of Life Skills Education in Kenya, Nairobi, Kenya: NAYA, 2012.
50. Mulama S, The sexuality education needs of teacher trainees in Kenya, Post-Sexuality Leadership Development Fellowship Report Series No. 5, 2002, http://www.arsrc.org/downloads/sldf/FinalReport%20Stella%20Mulama2006.p….
51. Birungi H et al., Education Sector Response to Early and Unintended Pregnancy: A Review of Country Experiences in Sub-Saharan Africa, STEP UP and UNESCO Research Report, 2015.
Suggested Citation
Sidze EM et al., From Paper to Practice: Sexuality Education Policies and Their Implementation in Kenya, New York: Guttmacher Institute, 2017, https://www.guttmacher.org/report/sexuality-education-kenya.
Acknowledgments
This report was written by Estelle M. Sidze, Stephen Mulupi, Caroline P. Egesa, Martin Mutua, Winstoun Muga and Chimaraoke O. Izugbara, all of the African Population and Health Research Center (APHRC); and Melissa Stillman, Sarah Keogh, Ellie Leong and Akinrinola Bankole, all of the Guttmacher Institute. It was edited by John Thomas, and Kathleen Randall oversaw production; both are at the Guttmacher Institute.
The authors thank the following individuals for insightful comments on an early draft: Nicole Haberland, Population Council; Judith Helzner, independent consultant; Jane Kamau, UNESCO Kenya; Paul Kuria, National Gender and Equality Commission; and Eunice Muthengi, Population Council Kenya. They also acknowledge the following colleagues for their review and comments: Benta Abuya, Caroline Kabiru and Joyce Mumah, all of APHRC; and Ann Biddlecom, Evert Ketting, Gustavo Suarez and Vanessa Woog, all of the Guttmacher Institute. In addition, the authors thank Christine Panchaud, independent consultant, for her contributions to the development and testing of study instruments and fieldwork training.
The authors greatly appreciate the members of the Advisory Committee for their technical support and guidance during the development of the project and for contributions to the policy recommendations: Jane Kamau, UNESCO Kenya; Andrew Mwanthi, Nairobi City County school health department; Francis Obare, Population Council Kenya; Albert Obuyi, Center for the Study of Adolescence in Kenya; and Olive Wambui, Kenya Institute of Curriculum Development. The authors acknowledge the logistical support of the Kenya Ministry of Education in Nairobi, Mombasa and Homa Bay counties.
This report was made possible by grants to the Guttmacher Institute from the Dutch Ministry of Foreign Affairs and the Swedish International Development Cooperation Agency (Sida). Core support provided to APHRC by Sida and the William and Flora Hewlett Foundation also assisted in the development of the study and this report. The findings and conclusions in this report are those of the authors and do not necessarily reflect positions and policies of the donors. The Guttmacher Institute gratefully acknowledges the unrestricted funding it receives from many individuals and foundations—including major grants from the William and Flora Hewlett Foundation and the David and Lucile Packard Foundation—which undergirds all of the Institute’s work.


