The Reproductive Health Impact Study (RHIS) is a multiyear comprehensive research initiative analyzing the effects of federal and state policy changes on publicly funded family planning care in the United States. The study, which focuses on Arizona, Iowa, New Jersey and Wisconsin, documents the impact of these policies over the period 2017−2022 on family planning service delivery and on patients who rely on this care. New Jersey was selected as a focus state for the RHIS in 2019 because it has a long-established family planning network and policies that are generally supportive of sexual and reproductive health. For the New Jersey study, the Guttmacher Institute is working with the New Jersey Family Planning League and other in-state research and policy partners.
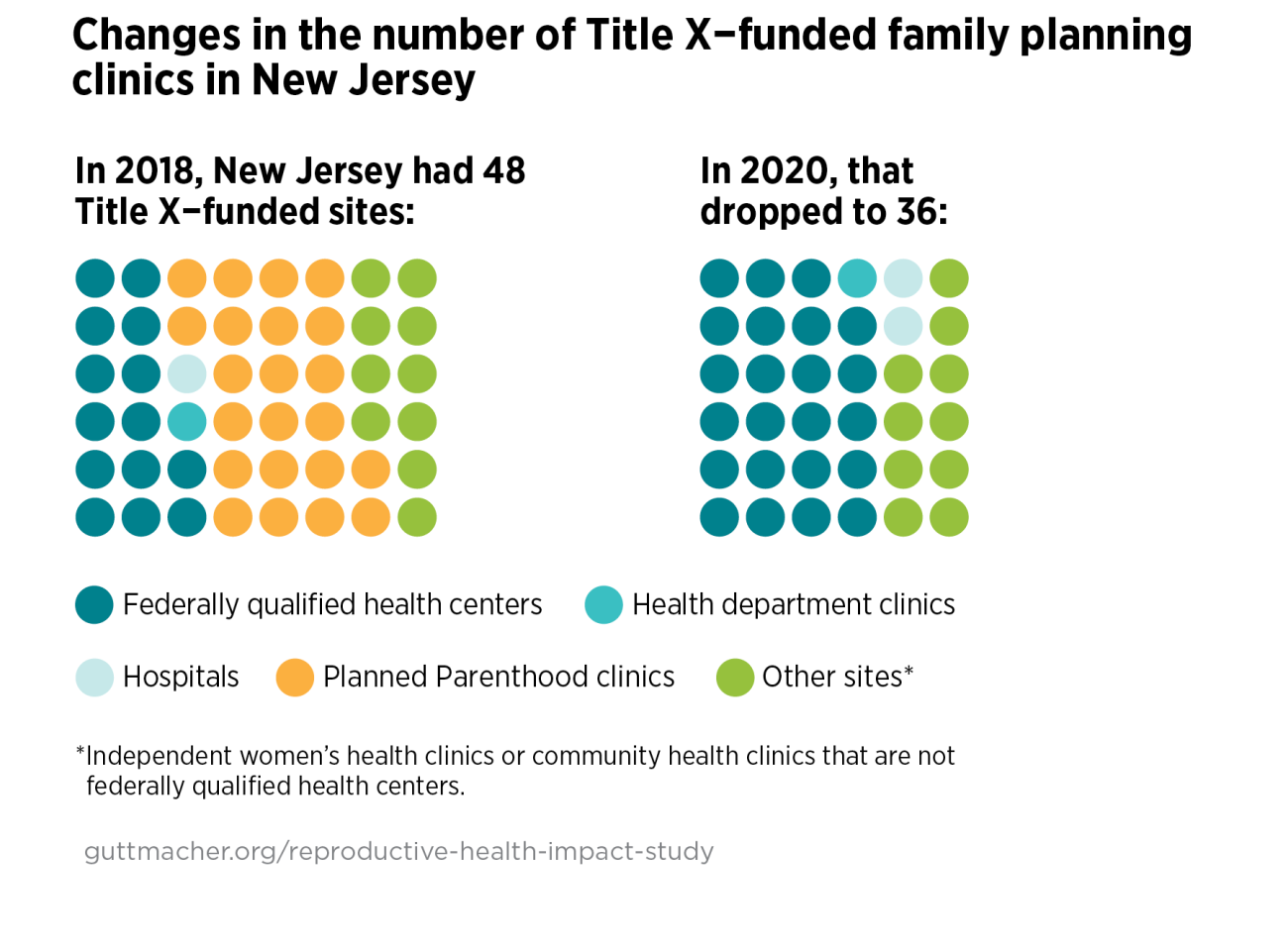
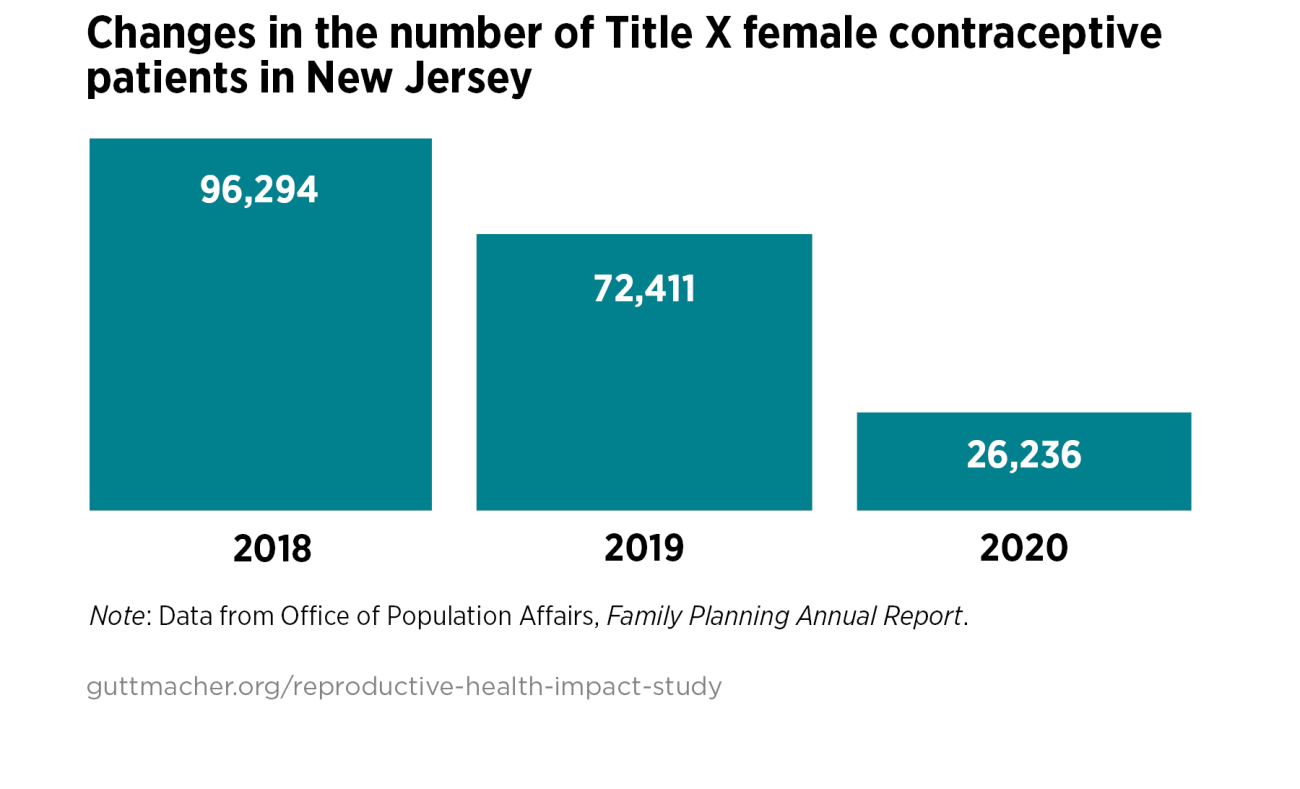
The RHIS was initially conceived in the aftermath of the 2016 election, in anticipation of federal and state efforts to change funding streams and service delivery for publicly funded family planning. As the study progressed, the RHIS team adapted ongoing study activities to document the impact of several events—notably, the 2019 changes to the federal Title X regulations (the Trump-Pence administration’s “domestic gag rule”) and the COVID-19 pandemic.
In March 2019, New Jersey was among 21 states that filed a lawsuit opposing the domestic gag rule. In early 2021, the Biden-Harris administration took the first step toward rescinding the domestic gag rule by signing a presidential memorandum directing the U.S. Department of Health and Human Services to review the rule and other restrictive Title X regulations and consider whether to suspend, revise or rescind them. In November 2021, the Biden-Harris administration’s Title X rule went into effect, restoring the crucial reproductive health care program to its previous state. The Biden-Harris rule revokes the 2019 Trump-Pence rule and updates regulations to focus on inclusion and health equity.
Ohio and 11 other states filed a lawsuit to block the Biden-Harris rule, which remains in effect while the case continues. New Jersey joined an amicus brief supporting the rule with 19 other states and the District of Columbia. In 2022, a federal court ruled in favor of the administration; the decision has been appealed. If the current rule is blocked, providers who left the Title X program as a result of the Trump-Pence gag rule might do so again. New Jersey is likely to appropriate state funds to cover family planning services if the Biden-Harris rule is blocked, as it did when the Trump-Pence rule was implemented.
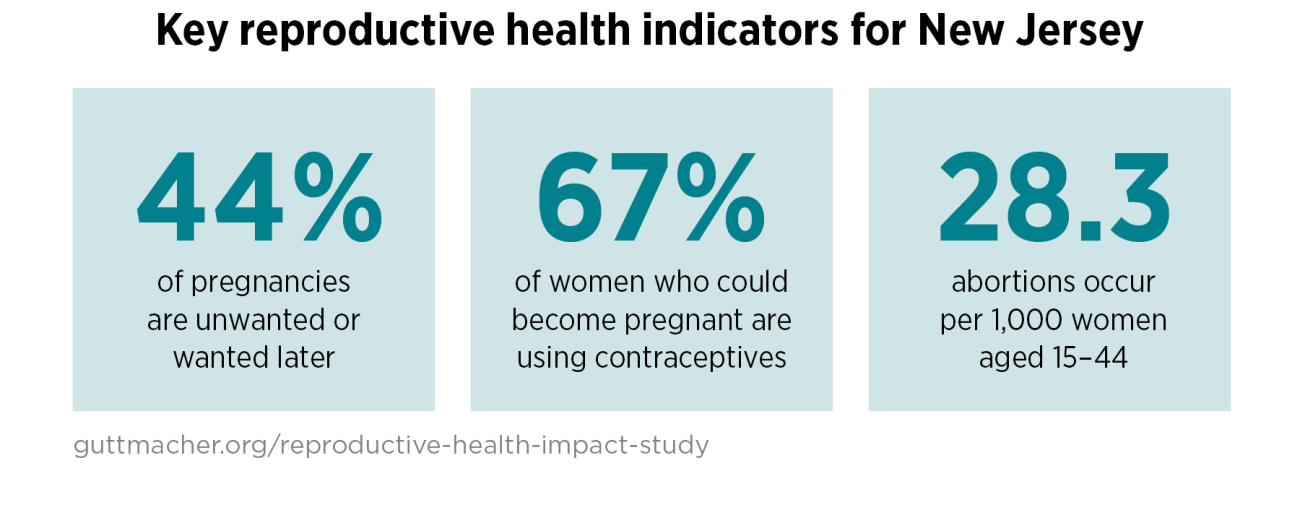
Some of the key reproductive outcomes for New Jersey residents that are being tracked in the study appear below. Documenting changes to these outcomes over the study period helps identify the effects of changes related to publicly funded family planning care in the state.